Abstract
Introduction: Hemoadsorption (HA) removes circulating inflammatory mediators and is used as an adjunct in septic shock. We assessed whether a protocol-based HA330 strategy improved early organ dysfunctions and outcomes.
Materials and Methods: We performed an observational study of adults with septic shock admitted to a 59-bed mixed ICU (January 2023–June 2024). We compared outcomes of patients who were treated with HA, to those who received standard of care alone.
Results: During the study period, 52 of 127 septic shock patients received hemoadsorption therapy (HA group), while 75 received standard care (control group). On ICU admission age, sex, comorbidity, APACHE II, and SOFA scores were similar. By day 3, SOFA score decreased with HA (8 [5–11] to 7 [5–9]; p<0.05) but was unchanged in controls. Vasoactive inotropic score declined in both groups, more prominently with HA. Mechanical ventilation requirement and ICU length of stay were comparable. AKI decreased from 71.2% to 46.2% in the HA but increased from 44.0% to 50.7% in the control group. Hospital stay was longer with HA (29,5 [18-47,75] vs 19 [12-30], p=0.009), whereas 28-day mortality was lower (30.8% vs 49.8%, p<0.05).
Conclusions: Protocol-based early HA at high vasopressor requirements was associated with improved organ dysfunctions and reduced 28-day mortality in septic shock patients.
Keywords: hemoadsorption, septic shock, vasoactive inotropic score, acute kidney injury, intensive care unit, mortality
Introduction
As per the Sepsis-3 definition, sepsis is a life-threatening organ dysfunction caused by dysregulated host response to infection (1). Sepsis represents a significant portion of all admissions in intensive care units (ICU) throughout the world. Septic shock, the most severe form of sepsis, is characterized by a need for vasopressors and elevated lactate levels and is associated with very high ICU mortality (1-5). Worldwide, sepsis is estimated to cause approximately 20 million deaths annually and account for 31.5% of all deaths (6). Sepsis associates an uncontrolled inflammatory response, cytokine storm, endothelial dysfunction, coagulopathy, and impairment in microcirculation (3). Standard management includes source identification, rapid broad-spectrum antimicrobial therapy, appropriate fluid resuscitation, and organ support. However, despite these therapies, the observed mortality remains very high. Hence, adjunct treatment strategies are required (7).
In recent years, hemoadsorption based therapies have been proposed as an adjunct treatment to the standard of care for sepsis or sepsis-like syndrome (8). The rationale is to remove harmful substances, such as excess cytokines, bacterial endotoxins and toxins, selectively or non-selectively from the circulation. The goal is to improve hemodynamics, reduce the need for vasopressor, preserve organ function, and ultimately decrease mortality (3,9). However, the evidence supporting the utilization of hemoadsorption in sepsis remains scarce and controversial. While some studies have reported a faster reduction in vasopressor dose (10,11), a decrease in inflammatory markers, and clinical improvement with HA treatment, some have not (12-14). Therefore, international guidelines currently do not recommend the routine use of hemoadsorption but encourage further investigations in selected patient groups (7).
Studies systematically examining the effect of hemoadsorption therapy on hemodynamic response, vasopressor requirement, lactate clearance, SOFA score, and organ functions are limited in number and have heterogeneous treatment protocols. Therefore, adequately designed clinical studies are needed to clarify the true clinical efficacy of hemoadsorption therapy, the patient groups likely to benefit from it, and the factors determining response to treatment.
In Türkiye, reimbursement for hemoadsorption (HA) by healthcare insurance was introduced in 2014. It was included in our institutions’ sepsis management protocol in 2021. However, due to budget restrictions, it was only available during certain periods of time. We sought to compare outcomes of patients with sepsis who received HA therapy (admitted during periods where the device was available) and controls (when it was not available at our center).
Materials and Methods
This observational cohort study was conducted in a 59-bed mixed ICU. Our center is a closed-unit ICU where extracorporeal therapies (extracorporeal membrane oxygenation (ECMO), hemodialysis, hemoadsorption, plasmapheresis) can be provided 24/7 by intensive care specialists, intensive care subspecialty residents, and anesthesiology and reanimation residents.
Study population: All adult (≥18 years) patients who met Sepsis-3 diagnostic criteria for septic shock and were admitted to our ICU for a duration of more than 24 hours were considered for inclusion in the study (1). We excluded pregnant or lactating women, patients with advanced malignancies and those with missing data. Patients who received hemoadsorption with the HA330 cartridge (HA group) were matched with septic patients who had similar APACHE II, SOFA, and age measurements at ICU admission but did not receive HA therapy (control group).
Standard of care
In our ICU, standard of care for sepsis corresponds to the Surviving Sepsis Campaign (SSC) international guidelines (7). Briefly, this includes, early recognition, identification and control of the source, obtaining appropriate cultures, initiation of broad-spectrum antibiotic therapy, fluid resuscitation with 30 mL/kg of crystalloid fluid and initiation of vasopressor (first choice norepinephrine) if mean arterial pressure (MAP) remained <65 mmHg despite fluid resuscitation. When norepinephrine dose exceeded 0.25 µg/kg/min or hemodynamic instability persisted despite increasing vasopressor requirements, hydrocortisone (200 mg/day) was added, and a second vasopressor agent started.
Hemoadsorption protocol
According to our protocol, hemoadsorption is considered in patients with sepsis, when despite all measures described above, the norepinephrine dose exceeds 0.20-0.25 µg/kg/min. This threshold is considered as indicative of refractory septic shock and of a high inflammatory response. When CRRT is applied, hemoadsorption therapy consists of the insertion of an HA 330 (Jafron Biomedical Co., Ltd., Zhuhai, China) cartridge within the CRRT device.When no CRRT is provided, similar cartridges are used but in hemoperfusion mode within a dedicated device. Once initiated, hemoadsorption therapy is administered once daily for an aimed duration of 3 days. Consistent with reports in which hemoperfusion sessions were extended up to 8 hours in selected settings (15) we used a treatment duration of approximately 6–8 hours, with flow rates ranging between 150 and 250 mL/min.
Data Collection: Eligible patients were identified and data retrieved from their electronic medical records as well as from daily ICU observation charts. Patients’ age, gender, body mass index, comorbid diseases, and admission diagnoses were recorded as well as clinical parameters and laboratory results obtained during ICU admission. We assessed acute kidney injury (AKI) presence and stage according to kidney disease: improving global outcomes (KDIGO). Glasgow coma scale (GCS), acute physiology and chronic health evaluation II (APACHE II), and sequential organ failure assessment score (SOFA) were calculated upon ICU admission. Initial AKI and vasoactive inotropic score (VIS) were calculated at the time septic shock was diagnosed, and then recalculated daily for the first three days. In addition, we recorded administered treatments (vasoactive drugs, antibiotics), interventions (mechanical ventilation, hemodialysis, hemoadsorption, plasmapheresis, ECMO) and complications. Finally, 28-day mortality was recorded.
Outcomes: Our primary outcome was 28-day mortality. Our secondary outcomes included ICU and hospital length of stay (LOS), duration of mechanical ventilation, changes in SOFA score, organ dysfunctions, as well as vasopressor and inotrope requirements.
Sample Size: Based on prior evidence, to detect a 23.6% reduction in ICU mortality associated with the intervention with 80% statistical power, a two-sided 95% confidence interval, and a 1:1 allocation ratio, a minimum of 48 patients per group was required (16).
Ethical Issues: The study was approved by Marmara University Medical Faculty Research and Ethics Committee (approval no: 09.2024.811). The research was conducted in conformity with the Declaration of Helsinki and Good Clinical Practice guidelines. As this study had a retrospective design and was based on the analysis of routinely collected, anonymized clinical data, informed consent from individual patients could not be obtained and the need for informed consent was therefore waived in accordance with current ethical guidelines.
Data evaluation and statistical analysis
Statistical analyses were performed using SPSS Statistics, version 22.0 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to assess the normality of distribution for continuous variables. Categorical variables are presented as counts and percentages. Continuous variables with a normal distribution are expressed as mean ± standard deviation, whereas non-normally distributed variables are expressed as median and interquartile range (IQR). Between-group comparisons of continuous variables were performed using the independent-samples t test for normally distributed data and the Mann–Whitney U test for non-normally distributed data. Within-group comparisons of continuous variables were conducted using the Wilcoxon signed-rank test. For the within-group analysis of more than two numerical variables, repeated-measures ANOVA was used; when the assumptions of this test were not met, the Friedman test was applied. Categorical variables were compared using the chi-square test or McNemar test, as appropriate; when the assumptions for the chi-square test were not met, Fisher’s exact test was applied. A two-sided p-value < 0.05 was considered statistically significant
Results
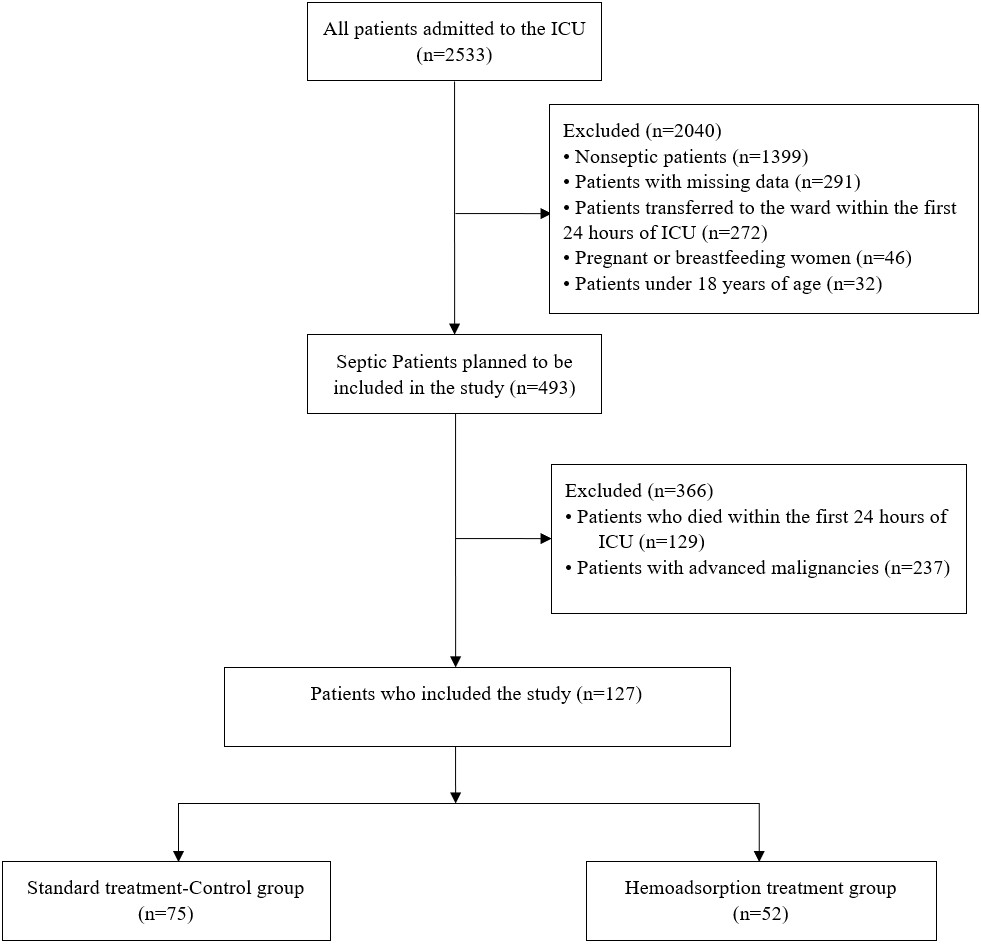
Patients: During the study period, 2533 patients were admitted to our unit. Of those, as shown in Figure 1, we excluded 1399 who had did not have sepsis, 32 who were <18 yo and 272 who stayed less than 24 hours in ICU, 46 who were pregnant or breastfeeding and 291 who missing data. In addition, another 366 were excluded from the analysis as they died within the first 24 hours (129) or had advanced malignancies (237). Hence, 127 were eligible to enter the study. Of these, 52 received hemoadsorption (HA group), and 75 did not (control group).
The two groups and their baseline characteristics are described in Table 1. Overall, there were no significant differences at baseline between the two groups sex, body mass index, Charlson comorbidity index. There were imbalances in the source of sepsis. Indeed, pulmonary infections were more frequent in the control group (58.7% vs. 23.1%, p<0.001), whereas bloodstream infections were more common in the HA group (26.9% vs. 8.0%, p<0.05). Gram-negative organisms tended to be more frequent in the HA group, and gram-positive organisms in the control group (Table 2).
| ICU: intensive care unit; APACHE: acute physiology and chronic health evaluation; GCS: Glasgow coma scale; SOFA: sequential organ failure assessment; VIS: vasoactive-inotropic score; SD: standard deviation; IQR: inter quartile range. | |||
| Table 1. Demographic characteristics, ICU disease severity scores and VIS score | |||
| Parameters |
(52; 40,9%) Median (IQR) |
(75; 59,1%) Median (IQR) |
|
| Age, mean±SD |
|
|
|
| Gender, n(%) |
|
||
| Male |
|
|
|
| Female |
|
|
|
| Body mass index, mean±SD (kg/m2) |
|
|
|
| Height |
|
|
|
| Weight |
|
|
|
| Charlson comorbidty index |
|
|
|
| ICU Scores | |||
| APACHE II |
|
|
|
| GCS first day |
|
|
|
| GCS 2. day |
|
|
|
| GCS 3. day |
|
|
|
| SOFA first day |
|
|
|
| SOFA 2. day |
|
|
|
| SOFA 3. day |
|
|
|
| VIS first day |
|
|
|
| VIS 2. day |
|
|
|
| VIS 3. day |
|
|
|
| Noradrenaline first day (mg/day) |
|
|
|
| Noradrenaline 2. day (mg/day) |
|
|
|
| Noradrenaline 3. day (mg/day) |
|
|
|
| Adrenaline first day (mg/day) |
|
|
|
| Adrenaline 2. day (mg/day) |
|
|
|
| Adrenaline 3. day (mg/day) |
|
|
|
| Adrenaline, n (%) |
|
|
|
| Terlipressin, n (%) |
|
|
|
| Methylen blue, n (%) |
|
|
|
| Steroid, n (%) |
|
|
|
| CRP: C-reactive protein, IQR: inter quartile range. | |||
| Table 2. Infection parameters | |||
| Enfection Parameters |
(52; 40,9%) Median (IQR) |
(75; 59,1%) Median (IQR) |
|
| Procalcitonin first day |
|
|
|
| Procalcitonin 2. day |
|
|
|
| Procalcitonin 3. day |
|
|
|
| CRP first day |
|
|
|
| CRP 2. day |
|
|
|
| CRP 3. day |
|
|
|
| Enfection sources, n (%) | |||
| Lung |
|
|
|
| Blood circulation |
|
|
|
| Urinary system |
|
|
|
| Central catheter |
|
|
|
| Central nervous system |
|
|
|
| Intraabdominal |
|
|
|
| Surgical site |
|
|
|
| Culture negative |
|
|
|
| Pozitive culture, n (%) | |||
| Gram negative | |||
| Acinetobacter baumannii |
|
|
|
| Klebsiella Pneumonia |
|
|
|
| Pseudomonas Aeruginosa |
|
|
|
| Other Gram negative |
|
|
|
| Gram positive | |||
| Staph Aureus |
|
|
|
| Streptococus pneumoniae |
|
|
|
| Other Gram positive |
|
|
|
| Fungal | |||
| Candida albicans |
|
|
|
| Candida auris |
|
|
|
| Other fungal |
|
|
|
Primary outcome: 28-day mortality
Compared with patients in the control group, patients in the HA group had a lower 28-day mortality (30.8 versus 49.3%, p = 0.037) (Table 3).
|
AKI: acute kidney injury; LOS: Length of stay, CRRT: Continuous renal replacement therapy, IQR: inter quartile range. a: 1. day versus lastday (p<0.05), b: 2. day versus lastday (p<0.05), c: 3. day versus lastday (p<0.05) |
|||
| Table 3. Acute kidney injury, CRRT rates, length of stay, and 28-day mortality | |||
| Parameters |
(52; 40,9%) n (%) |
(75; 59,1%) n (%) |
|
| AKI first day |
|
|
|
| AKI 2. day |
|
|
|
| AKI 3. day |
|
|
|
| AKI last day |
|
|
|
| AKI stage first day |
|
||
| Non-AKI |
|
|
|
| AKI stage 1 |
|
|
|
| AKI stage 2 |
|
|
|
| AKI stage 3 |
|
|
|
| AKI stage 2. day |
|
||
| Non-AKI |
|
|
|
| AKI stage 1 |
|
|
|
| AKI stage 2 |
|
|
|
| AKI stage 3 |
|
|
|
| AKI stage 3. day |
|
||
| Non-AKI |
|
|
|
| AKI stage 1 |
|
|
|
| AKI stage 2 |
|
|
|
| AKI stage 3 |
|
|
|
| AKI lastday |
|
||
| Non-AKI |
|
|
|
| AKI stage 1 |
|
|
|
| AKI stage 2 |
|
|
|
| AKI stage 3 |
|
|
|
| CRRT |
|
|
|
| CRRT total days, median (IQR) |
|
|
|
| Length of stay | |||
| ICU LOS, day median(IQR) |
|
|
|
| Hospital LOS, day median(IQR) |
|
|
|
| Mortality | |||
| 28 day mortality |
|
|
|
Secondary outcomes
Clinical outcomes
Compared with the control group, patients in the HA group had similar ICU LOS but longer hospital LOS (21 vs 13, p=0.079 and 29.5 vs 19, p=0.009, respectively). The duration of mechanical ventilation was determined to be 13 (5.5-31.5) days in the HA group and 10 (7-19) days in the control group (p>0.05) (Table 4).
| FiO2: fraction of inspired oxygen; PEEP: positive end-expiratory pressure; PS: pressure support; PaO2/FiO2: partial pressure of oxygen/ fraction of inspired oxygen; IQR: inter quartile range. | |||
| Table 4. Mechanical ventilation and blood gas parameters | |||
| Parameters |
(52; 40,9%) Median (IQR) |
(75; 59,1%) Median (IQR) |
|
| Mechanical ventilation and blood gas parameters | |||
| Mechanical ventilation, n(%) |
|
|
|
| Mechanical ventilation duration (day) |
|
|
|
| FiO2 (%) first day |
|
|
|
| FiO2 (%) 2. day |
|
|
|
| FiO2 (%) 3. day |
|
|
|
| PEEP first day |
|
|
|
| PEEP 2. day |
|
|
|
| PEEP 3. day |
|
|
|
| PS first day |
|
|
|
| PS 2. day |
|
|
|
| PS 3. day |
|
|
|
| PaO2/FiO2 ratio first day |
|
|
|
| PaO2/FiO2 ratio 2. day |
|
|
|
| PaO2/FiO2 ratio 3. day |
|
|
|
| Ph first day |
|
|
|
| Ph 2. day |
|
|
|
| Ph 3. day |
|
|
|
| Lactate first day |
|
|
|
| Lactate 2. day |
|
|
|
| Lactate 3. day |
|
|
|
Organ dysfunctions
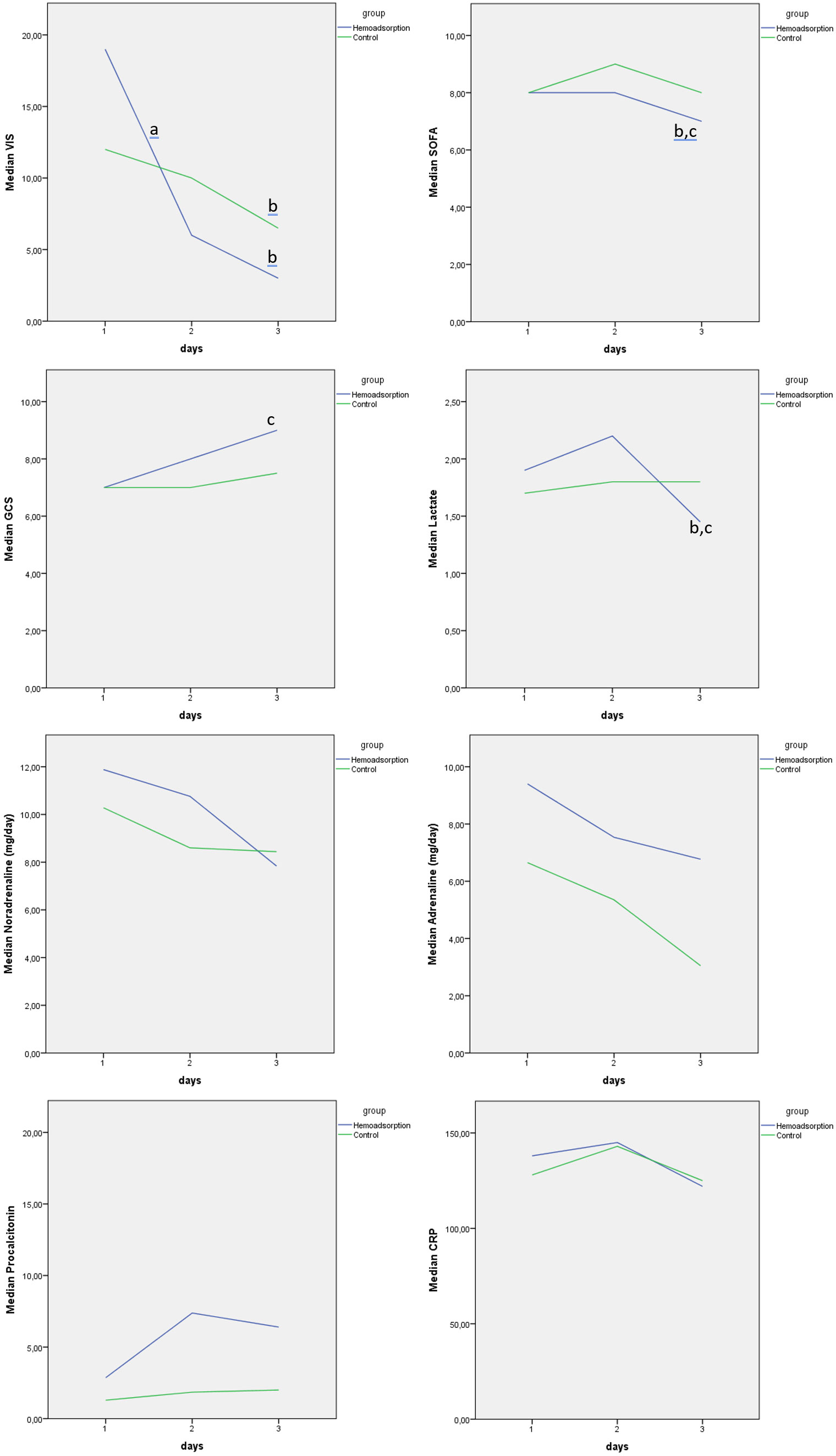
As shown in Figure 2, SOFA scores were similar between the two groups on days 1 and 2, but lower on day 3 in the HA group (7 [5-9] versus 8 [6-11], (p<0.05).
Within 72 hours of ICU admission, there was no difference between the two groups in terms of VIS Score, noradrenaline or adrenaline doses or the proportions of patients receiving adrenaline, methylene blue, terlipressin, and steroids (Table 1). Similarly, there was no difference in terms of MAP or heart rate (Table 5).
|
MAP: mean arterial pressure; SD: standard deviation; IQR: inter quartile range. a: 1. day versus 2.day (p<0.05), b: 1. day versus 3.day (p<0.05), c: 2. day versus 3.day (p<0.05) |
|||
| Table 5. Hemodynamic monitoring and laboratory parameters | |||
| Parameters |
(52; 40,9%) Median (IQR) |
(75; 59,1%) Median (IQR) |
|
| MAP min first day |
|
|
|
| MAP min 2. day |
|
|
|
| MAP min 3. day |
|
|
|
| MAP max first day |
|
|
|
| MAP max 2. day |
|
|
|
| MAP max 3. day |
|
|
|
| Heart rate min first day, mean±SD |
|
|
|
| Heart rate min 2. day, mean±SD |
|
|
|
| Heart rate min 3. day, mean±SD |
|
|
|
| Heart rate max firstday, mean±SD |
|
|
|
| Heart rate max 2. day, mean±SD |
|
|
|
| Heart rate max 3. day, mean±SD |
|
|
|
| Hemoglobin first day |
|
|
|
| Hemoglobin 2. day |
|
|
|
| Hemoglobin 3. day |
|
|
|
| Platelet firstday |
|
|
|
| Platelet 2. day |
|
|
|
| Platelet 3. day |
|
|
|
| Leukocyte first day |
|
|
|
| Leukocyte 2. day |
|
|
|
| Leukocyte 3. day |
|
|
|
| Lymphocyte first day |
|
|
|
| Lymphocyte 2. day |
|
|
|
| Lymphocyte 3. day |
|
|
|
| Bilirubin firstday |
|
|
|
| Bilirubin 2. day |
|
|
|
| Bilirubin 3. day |
|
|
|
| Creatinine first day |
|
|
|
| Creatinine 2. day |
|
|
|
| Creatinine 3. day |
|
|
|
| Input firstday |
|
|
|
| Input 2. day |
|
|
|
| Input 3. day |
|
|
|
| p value (Input within-group analysis) |
|
|
|
| Output firstday |
|
|
|
| Output 2. day |
|
|
|
| Output 3. day |
|
|
|
| p value (Output within-group analysis) |
|
|
|
| Balance first day |
|
|
|
| Balance 2. day |
|
|
|
| Balance 3. day |
|
|
|
| p value (Balance within-group analysis) |
|
|
|
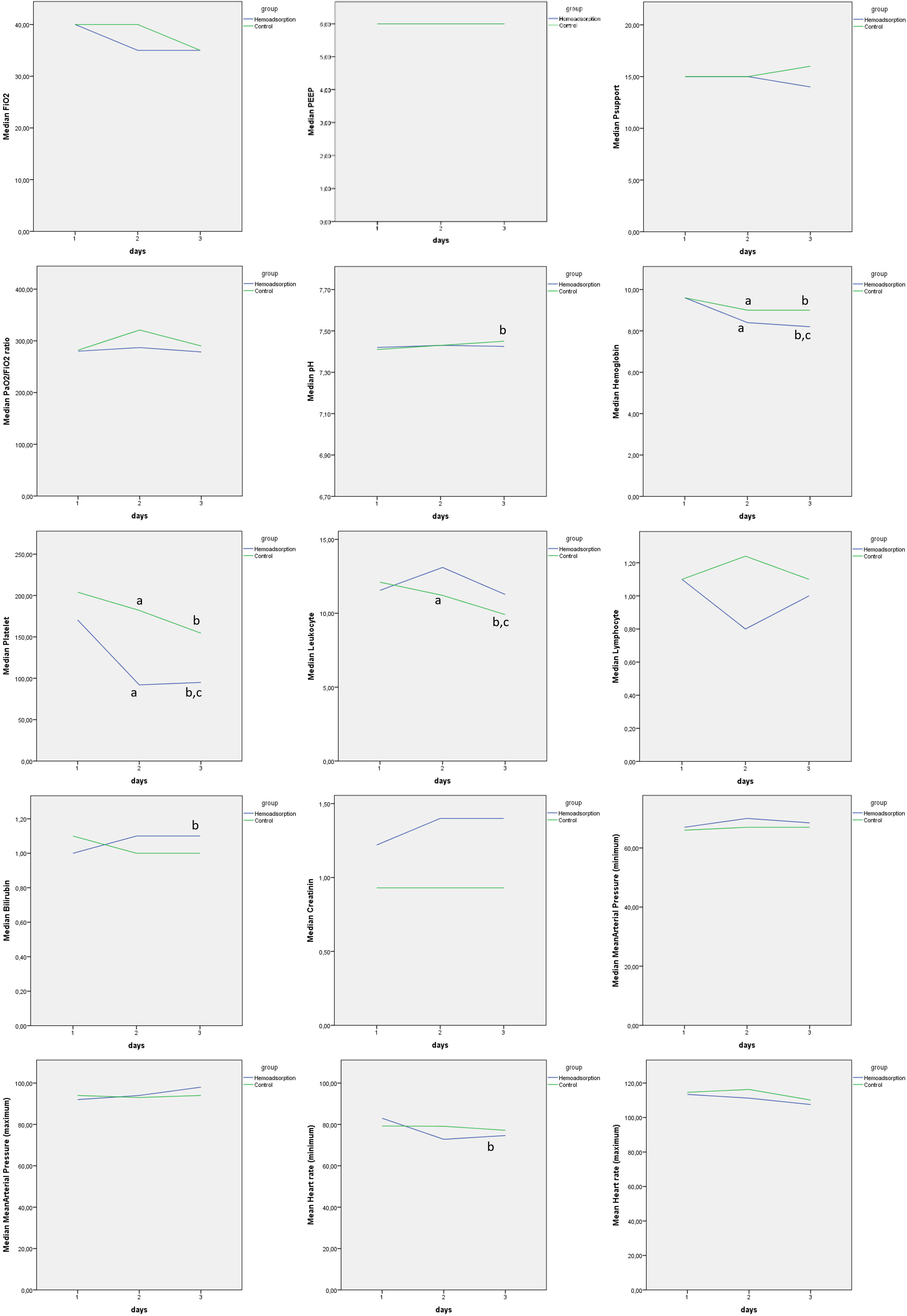
The proportion of patients requiring mechanical ventilation was similar (94.2% vs 93.3%), in the two groups. There was no difference between the two groups in terms of FiO2, PEEP, pressure support values, PaO2/FiO2 ratios. Arterial blood gas analyses showed no between-group differences in pH, lactate, or other parameters (p>0.05). In the within-group analysis, a significant decrease in lactate level was observed in the HA group on day 3 (1.5 [1.1–2.2]) compared with day 1 (1.9 [1.3–3.9]) and day 2 (2.2 [1.2–4.1]), whereas no significant change in lactate was detected in the control group (Figure 2).
There was no difference in terms of GCS scores.
Acute kidney injury (AKI) was significantly more common in the HA group on day 1 (71.2% vs. 44.0%, p<0.05). However, the proportion was similar in the two groups on days 2 and 3 as well as on ICU discharge (46.2% vs. 50.7%, p>0.05) (Table 3). In the within-group analysis, AKI rates remained stable across day 1, day 2, day 3, and the last ICU day in the control group, whereas in the HA group the AKI rate on the last ICU day was significantly lower than on each of the first three days. No between-group differences in creatinine levels were observed. Fluid balance over the three-day period was similar in both groups (Table 4). CRRT use was significantly higher in the HA group (71.2% vs. 26.7%, p<0.001), and CRRT duration was longer in the HA group (p<0.05).
Hemoglobin level on day 3 was significantly lower in the HA group (8.2 [7.8–9.6]) compared with the control group (9.0 [8.2–10.1]) (p<0.05). Platelet counts were lower in the HA group from day 1 onwards, and this difference was statistically significant on days 2 and 3 (Figure 3). Within groups, platelet counts decreased significantly in both arms, with a more marked decline in the HA group (p<0.001).
Procalcitonin levels were significantly higher in the HA group on days 2 and 3 (day 2: 7.38 [2.65–24.86] vs. 1.85 [0.29–6.16]; day 3: 6.40 [2.98–25.54] vs. 2.0 [0.28–7.76]; p<0.001 for both). No difference was observed between groups in CRP levels.
Discussion
We conducted a matched control study to evaluate the effect of hemoadsorption in patients with septic shock requiring more than 0.2 mcg/kg/min of noradrenaline. We found that, despite a higher infection burden and a greater frequency of AKI in patients receiving HA, the intervention was associated with a lower 28-day mortality rate compared with patients receiving conventional therapy. The length of hospital stay was longer in the HA group, which may be explained by the lower mortality in this group compared with the control group. The intervention was associated with a lower SOFA score on day 3. There was no other difference in terms of physiological parameters except for a mild decrease in hemoglobin and a significant decrease in platelet count.
The lower mortality observed in the HA group is particularly noteworthy given the conflicting results in the literature (14). Although randomized controlled trials have reported no significant effect of hemoadsorption on mortality (13,14), observational studies in septic shock patients with a high inflammatory burden have described improvements in survival (10,11,17,18). This variability may be related to differences in patient selection, sepsis severity, and timing of treatment initiation. In our cohort, the observation that treated patients had a lower mortality rate despite a more severe baseline profile suggests that the timing of hemoadsorption may play a critical role in clinical outcomes. Specifically, initiating treatment at the refractory shock stage, defined as a norepinephrine dose >0.20-0.25 µg/kg/min may partly explain the mortality difference observed in our study.
VIS has been validated as an independent predictor of mortality in adult patients with septic shock; higher mean and peak VIS values in the first 48 hours are strongly associated with non-survival (19). With regard to hemodynamic response, the absence of a significant difference between groups in VIS, norepinephrine, and adrenaline doses over the first three days is an expected finding and aligns with previous reports indicating that hemoadsorption may not lead to a dramatic reduction in vasopressor requirements within the first 24–72 hours (8,13).
Hemoadsorption was associated with a decrease in SOFA scores by day 3. This is consistent with reports of improved organ function by reducing inflammatory load with hemoadsorption (3,9). In addition, the reduction in vasopressor requirement together with the decrease in inflammatory burden may have improved vascular tone and tissue perfusion, thereby supporting organ recovery. The significant decrease in lactate levels in the HA group, as an indicator of improved microcirculation and perfusion, further reinforces this interpretation.
A larger proportion of patients from the HA group had AKI on day 1 and ultimately required CRRT. However, this difference disappeared over the 3 days follow-up suggesting a beneficial effect of hemoadsorption on renal dysfunction. This finding is consistent with studies indicating that hemoadsorption may help preserve renal perfusion by removing endotoxins and proinflammatory cytokines (3,9). Lower ICU or 30-day mortality were also observed in cohorts of patients with septic shock and AKI requiring CRRT when hemoadsorption was administered. (20) Such improvements in organ function, including AKI and liver dysfunction, may translate into better long-term survival (13), although this remains to be demonstrated. (21,22)
The higher procalcitonin levels in the HA group on days 2 and 3 is unexpected. It might potentially be explained by a different type of infection foci. Indeed, bloodstream infections were more frequent in the HA group, whereas pulmonary infections were more common in the control group.
Interpretation
Altogether, our findings indicate that hemoadsorption may be beneficial when applied to the appropriate patient population at an appropriate time point in the disease course. The potential of hemoadsorption to improve survival appears particularly relevant in cases with a high infection load, refractory shock, and rapidly evolving organ dysfunction.
The observed longer length of hospital stay in the HA group, may be explained by the lower mortality in this group compared with the control group.
Strengths and limitations
One of the main strengths of this study is the evaluation of hemoadsorption therapy using a large, detailed dataset of critically ill patients with septic shock. A thorough analysis of hemodynamic, laboratory, and organ function parameters was performed. In addition, strict adherence to the Surviving Sepsis Campaign guidelines in both groups enabled a reliable evaluation of the incremental contribution of hemoadsorption within a standardized treatment framework. Importantly, the use of a protocol-based HA strategy in our unit strengthens the internal validity and interpretability of the findings.
However, the study also has limitations to be acknowledged. First, its retrospective design precludes definitive conclusions about causality and does not fully eliminate the risk of selection bias. However, we have performed careful matching to identify a control group with similar baseline characteristics. Second, the single-center setting may limit the generalizability of the findings, as patient characteristics and treatment protocols may reflect local practice patterns. Thirdly, residual confounding may be present, as suggested by the higher incidence of AKI on day 1 and higher procalcitonin levels in the HA group. However, this should bias our results against the intervention, overall strengthening our main result. Finally, the lack of long-term follow-up data, such as renal function, readmission rates, or health-related quality of life, limits our ability to evaluate the late effects of hemoadsorption therapy.
Conclusion
Early protocol based hemoadsorption was associated with an improved 28 days mortality, a decrease SOFA score in critically ill patients with septic shock. These results should be confirmed in prospective, randomized controlled trials.
Ethical approval
The study was approved by the Marmara University Medical Faculty Research and Ethics Committee (09.2024.811). Informed consent was not obtained due to retrospective nature of the study
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:801-10. https://doi.org/10.1001/jama.2016.0287
- Gül F, Arslantaş MK, Cinel İ, Kumar A. Changing definitions of sepsis. Turk J Anaesthesiol Reanim. 2017;45:129-38. https://doi.org/10.5152/TJAR.2017.93753
- Jarczak D, Kluge S, Nierhaus A. Sepsis-pathophysiology and therapeutic concepts. Front Med (Lausanne). 2021;8:628302. https://doi.org/10.3389/fmed.2021.628302
- Vincent JL, Marshall JC, Namendys-Silva SA, et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. 2014;2:380-6. https://doi.org/10.1016/S2213-2600(14)70061-X
- Vincent JL, Sakr Y, Sprung CL, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34:344-53. https://doi.org/10.1097/01.ccm.0000194725.48928.3a
- GBD 2021 Global Sepsis Collaborators. Global, regional, and national sepsis incidence and mortality, 1990-2021: a systematic analysis. Lancet Glob Health. 2025;13:e2013-26. https://doi.org/10.1016/S2214-109X(25)00356-0
- Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47:1181-247. https://doi.org/10.1007/s00134-021-06506-y
- Bottari G, Ranieri VM, Ince C, et al. Use of extracorporeal blood purification therapies in sepsis: the current paradigm, available evidence, and future perspectives. Crit Care. 2024;28:432. https://doi.org/10.1186/s13054-024-05220-7
- Malard B, Lambert C, Kellum JA. In vitro comparison of the adsorption of inflammatory mediators by blood purification devices. Intensive Care Med Exp. 2018;6:12. https://doi.org/10.1186/s40635-018-0177-2
- Kogelmann K, Jarczak D, Scheller M, Drüner M. Hemoadsorption by CytoSorb in septic patients: a case series. Crit Care. 2017;21:74. https://doi.org/10.1186/s13054-017-1662-9
- Schultz P, Schwier E, Eickmeyer C, Henzler D, Köhler T. High-dose CytoSorb hemoadsorption is associated with improved survival in patients with septic shock: A retrospective cohort study. J Crit Care. 2021;64:184-92. https://doi.org/10.1016/j.jcrc.2021.04.011
- Abdullayev R, Gul F, Bilgili B, Seven S, Cinel I. Cytokine adsorption in critically ill COVID-19 patients, a case-control study. J Intensive Care Med. 2022;37:1223-8. https://doi.org/10.1177/08850666221085185
- Schädler D, Pausch C, Heise D, et al. The effect of a novel extracorporeal cytokine hemoadsorption device on IL-6 elimination in septic patients: a randomized controlled trial. PLoS One. 2017;12:e0187015. https://doi.org/10.1371/journal.pone.0187015
- Becker S, Lang H, Vollmer Barbosa C, Tian Z, Melk A, Schmidt BMW. Efficacy of CytoSorb®: a systematic review and meta-analysis. Crit Care. 2023;27:215. https://doi.org/10.1186/s13054-023-04492-9
- Abbasi S, Naderi Z, Amra B, et al. Hemoperfusion in patients with severe COVID-19 respiratory failure, lifesaving or not? J Res Med Sci. 2021;26:34. https://doi.org/10.4103/jrms.JRMS_1122_20
- Premužić V, Babel J, Gardijan D, et al. Extracorporeal blood purification is associated with improvement in biochemical and clinical variables in the critically-ill COVID-19 patients. Ther Apher Dial. 2022;26:316-29. https://doi.org/10.1111/1744-9987.13730
- Brouwer WP, Duran S, Kuijper M, Ince C. Hemoadsorption with CytoSorb shows a decreased observed versus expected 28-day all-cause mortality in ICU patients with septic shock: a propensity-score-weighted retrospective study. Crit Care. 2019;23:317. https://doi.org/10.1186/s13054-019-2588-1
- Rugg C, Klose R, Hornung R, et al. Hemoadsorption with CytoSorb in septic shock reduces catecholamine requirements and in-hospital mortality: a single-center retrospective ‘genetic’ matched analysis. Biomedicines. 2020;8:539. https://doi.org/10.3390/biomedicines8120539
- Kara İ, Sargın M, Bayraktar YŞ, Eyiol H, Duman İ, Çelik JB. The use of vasoactive-inotropic score in adult patients with septic shock in intensive care. J Crit Intensive Care. 2019;10:23-30. https://doi.org/10.33381/dcbybd.2019.2057
- Epstein D, Badarni K, Bar-Lavie Y. Impact of haemoadsorption therapy on short term mortality and vasopressor dependency in severe septic shock with acute kidney injury: a retrospective cohort study. Antibiotics (Basel). 2024;13:1233. https://doi.org/10.3390/antibiotics13121233
- Hellman T, Uusalo P, Järvisalo MJ. Renal replacement techniques in septic shock. Int J Mol Sci. 2021;22:10238. https://doi.org/10.3390/ijms221910238
- Şenol EA, Karakoç E, Göçerler Z, Aydın OÖ, Yelken B. The efficacy of continuous renal replacement therapy and hemoabsorption treatments in COVID-19 patients in the intensive care unit: a retrospective evaluation. Turk J Intensive Care 2023;21:181-9. https://doi.org/10.4274/tybd.galenos.2022.30932
Copyright and license
Copyright © 2025 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.