
Abstract
Objective: This study aimed to investigate the prognostic value of the Charlson comorbidity index (CCI), American Society of Anesthesiologists (ASA) status, and Acute Physiology and Chronic Disease Evaluation II (APACHE-II) score in critically ill geriatric hip fracture patients followed in the surgical intensive care unit (SICU).
Materials and Methods: Critical geriatric hip fracture patients who underwent surgery and were followed in the SICU between January 2022 and December 2023 were evaluated retrospectively. The performance of CCI, ASA status, and APACHE-II scores in predicting in-hospital mortality was investigated.
Results: The study included 137 patients, and 66.4% (n=91) were female. ASA IV status, APACHE-II, CCI score, and the number of patients with coronary vascular disease/heart failure were significantly higher in the mortality group (p=0.003, p<0.001, p<0.001, and 0.010, respectively). Mean Glasgow Coma Scale and serum albumin levels at SICU admission were significantly lower in the mortality group (p=0.008 and p=0.006, respectively). ASA status, APACHE-II, and CCI scores were independent predictors of mortality (p=0.002, p=0.022, and p=0.034, respectively). In ROC curve analysis, the area under the curve (AUC) for APACHE-II was 0.803 (95% CI, 0.697-0.908), AUC for CCI was 0.742 (95% CI, 0.598-0.886), and AUC for ASA status was 0.614 (0.458-0.769).
Conclusions: CCI, ASA status, and APACHE-II scores independently predict in-hospital mortality in patients with critical hip fractures. It has prognostic value in predicting mortality and is listed from highest to lowest as APACHE-II, CCI, and ASA status.
Keywords: hip fracture, Charlson comorbidity index, ASA, APACHE-II, in-hospital mortality
Introduction
Hip fractures are a leading cause of morbidity and mortality in the geriatric population (≥65 years). It is also among the top 10 causes of disability-adjusted life years lost for older adults (1). The proportion of the geriatric population is increasing rapidly in developed and developing countries due to increasing life expectancy and decreasing birth rates. According to the 2022 data from the Turkish Statistical Institute, the proportion of the geriatric population (≥ 65 years) in Turkey has increased to 9.9% (2). Visual and hearing impairments, decreased muscle strength and activity, decreased bone density and joint flexibility, decreased motor and cognitive functions, comorbidities, and polypharmacy in the geriatric population increase the risk of trauma (3). The most common mechanism of traumatic injury in geriatric patients is falls from ground level, and hip fractures occur frequently (4-6). The mortality rate in patients with hip fractures within the first year was reported as 21.9% in women and 32.5% in men (7). Deaths following hip fractures in the geriatric population are often due to cardiovascular and respiratory complications. Mortality rates increase in patients who develop pneumonia, pulmonary embolism, arrhythmias, and acute cardiovascular collapse. Critical geriatric hip fracture patients are frequently monitored in the intensive care unit (ICU) in the early postoperative period.
Prognostic scoring systems help predict mortality and plan aggressive treatment in critically ill patients followed in the ICU. Anesthesiologists frequently use the American Society of Anesthesiologists (ASA) status to determine preoperative physical status. However, the Acute Physiology and Chronic Disease Evaluation-II (APACHE-II) score helps predict mortality in patients admitted to the ICU. Scoring systems such as the Glasgow coma scale (GCS) and the revised trauma score, specific to trauma patients, have been reported to have prognostic value in critical trauma patients (6). Charlson comorbidity index (CCI) is a scoring system with prognostic value that considers patients’ age and chronic diseases. CCI has prognostic value in various clinical conditions and helps predict 30-day and 1-year mortality in patients with hip fractures (8-10).
This study compared the performances of CCI, ASA status, and APACHE-II scores in predicting in-hospital mortality in critically ill geriatric hip fracture patients who were followed up and treated postoperatively in a tertiary hospital’s surgical ICU (SICU).
Materials and Methods
This comprehensive retrospective observational study was conducted according to the principles of the Declaration of Helsinki. It was initiated after approval from the Clinical Research Ethics Committee of University of Health Sciences, Istanbul Kanuni Sultan Süleyman Training and Research Hospital (date: 08.05.2024, KAEK/2024.05.89). The study included patients who underwent surgery for geriatric hip fractures at the University of Health Sciences, Istanbul Kanuni Sultan Süleyman Training and Research Hospital between January 2021 and December 2023 and were followed up in the SICU during the postoperative period. Patient data were accessed through the hospital information system and patient files.
Inclusion criteria: Patients aged 65 years and older who underwent surgery due to geriatric hip fracture and were followed up in the SICU postoperatively. Exclusion criteria: (1) trauma to another extremity or body part in addition to hip fracture; (2) viral and bacterial infection within the last month; (3) deterioration and admission to the SICU while being followed up in the inpatient service postoperatively, (4) intraoperative cardiovascular arrest (5) missing data.
Our hospital, a tertiary healthcare institution, provides postoperative surgical intensive care unit (SICU) care with eight beds. Geriatric hip fracture patients with ASA III status or higher who are at high risk for cardiac, respiratory, or other systemic conditions are monitored in the SICU postoperatively. Patients who are not at high risk but who exhibit hemodynamic instability, cardiac, or respiratory failure during the perioperative period are also monitored in the SICU at the discretion of the anesthesiologist. The current study did not standardize SICU admission criteria. Patients deemed high risk during the preanesthetic visit or those identified as having hemodynamic instability during the intraoperative period and requiring close monitoring were admitted to the SICU.
The data collected, including demographic data, ASA status, comorbidities, CCI, Glasgow Coma Scale (GCS) and Acute Physiology and Chronic Disease Evaluation-II (APACHE-II) scores at the time of admission to SICU, anesthesia methods, SICU and hospital stay, hemoglobin and albumin levels at admission, and in-hospital mortality, is of utmost importance in understanding critical care outcomes. These findings were then categorized into a survivor group and a mortality group based on in-hospital mortality, a significant factor in critical care outcomes.
Charlson comorbidity index (CCI)
Charlson et al. developed the Charlson Comorbidity Index in 1987 to classify comorbidities that may affect the risk of death. The CCI is the most widely used comorbidity index to determine survival (1 year and 10 years) in patients with comorbidities (8). Each comorbidity is scored 1, 2, 3, or 6. The scores are added to provide a total score to predict mortality. As the CCI score increases, the patient’s mortality risk increases.
Comorbid diseases and corresponding scores in the CCI are listed below:
1 points each: Cerebrovascular disease, chronic lung disease, congestive heart failure, dementia, diabetes (under control), liver disease (mild), myocardial infarction, peptic ulcer disease, peripheral vascular disease, rheumatologic disease.
2 points each: Diabetes (uncontrolled, end organ damage present), hemiplegia and paraplegia, kidney disease, leukemia, lymphoma, malignancy (localized).
3 points each: Moderate or severe liver disease
6 points each: AIDS, metastatic malignancy
The following points are added to the CCI score of patients aged 50 and over:
Age 50 to 59: +1 point added
Age 60 to 69: +2 points added
Age 70 to 79: +3 points added
Age 80 and above: +4 points added.
The study’s primary objective was to compare the performance of CCI, ASA status, and APACHE-II scores in predicting in-hospital mortality in patients with geriatric hip fractures who were followed in the SICU. The sample size was not determined in this retrospective cohort study, and all patients who met the inclusion and exclusion criteria during the study’s two years were included.
Statistical analysis
All analyses were performed using SPSS v27.0 software (SPSS Inc., Chicago, USA). The conformity of the data to normal distribution was evaluated using the Shapiro-Wilks test, histogram, skewness, and kurtosis. Descriptive statistics were expressed as number of patients, percentage, and median (interquartile range = Q1-Q3). Mann-Whitney U test and independent samples t-test were used in the analysis of quantitative data. Qualitative data were analyzed using the Pearson chi-square test and Fisher exact test. Multivariate logistic regression analysis was performed to determine independent predictors that effectively predict mortality. Receiver operating characteristics (ROC) curve analysis was performed to determine the prognostic value of CCI, ASA status, and APACHE-II score. Statistical significance was set at p < 0.05.
Results
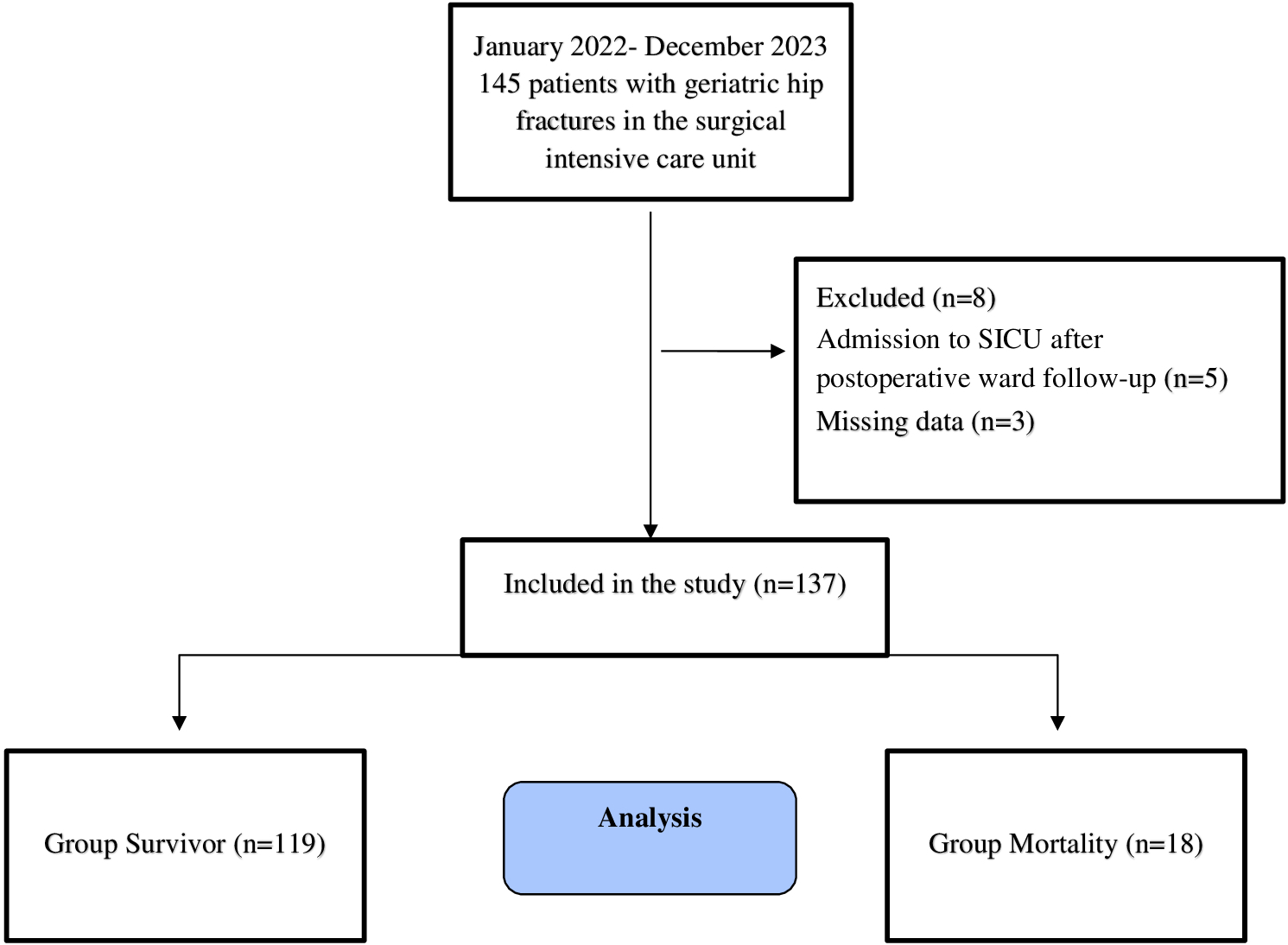
Between June 2021 and December 2023, 137 patients aged 65 years and older who underwent surgery (hemiarthroplasty and proximal femoral nail) due to hip fracture and were followed up in the SICU after surgery were included in the study (Figure 1). The mean age in the entire population was 79.1±8.4 years, and 66.4% (n=91) were female. Age, gender, and BMI did not differ significantly between the groups (p=0.692, p=0.113, and p=0.786, respectively). The mean GCS scores on admission to the SICU were significantly lower in the mortality group (11.7±2.7 vs. 13.7±1.5, p=0.008). The number of ASA IV patients was significantly higher in the mortality group (27.8% vs. 5%, p=0.003). The mean APACHE-II score at admission to the SICU was significantly higher in the mortality group than in the survival group (20.1±6.4 vs. 13.9±4.3, p<0.001). CCI was significantly higher in the mortality group (5.9±1.4 vs. 4.8±1.2, p<0.001). Spinal anesthesia was performed in 84.7% (n=116) of geriatric hip fracture patients, and the type of anesthesia did not differ significantly between the groups (p=0.211). At admission to the SICU, the mean hemoglobin values were lower in the mortality group, but no significant difference was observed (p=0.056). The mean ICU stay for the entire population was 4.1±6.5 days, and the mean hospital stay was 7.7±6.7 days. The in-hospital mortality rate for the entire population was 13.1% (Table 1).
| GCS: Glasgow Coma Scale, ASA: American Society of Anesthesiologist, APACHE-II: Acute Physiology and Chronic Health Assessment-II, CCI: Charlson Comorbidity Index, SICU: Surgical Intensive Care Unit. | ||||
| Table 1. Clinical characteristics. | ||||
| Variable |
|
|
|
|
| Age (years) |
|
|||
| Mean ± S.D |
|
|
|
|
| Median (Q1-Q3) |
|
|
|
|
| Age (range) |
|
|||
| 65-74 |
|
|
|
|
| 75-84 |
|
|
|
|
| ≥ 85 |
|
|
|
|
| Sex, n (%) |
|
|||
| Female |
|
|
|
|
| Male |
|
|
|
|
| Body mass index |
|
|||
| Mean±S.D |
|
|
|
|
| Median (Q1-Q3) |
|
|
|
|
| GCS |
|
|||
| Mean ± S.D |
|
|
|
|
| Median (Q1-Q3) |
|
|
|
|
| ASA status |
|
|||
| II |
|
|
|
|
| III |
|
|
|
|
| IV |
|
|
|
|
| APACHE-II |
|
|||
| Mean ± S.D |
|
|
|
|
| Median (Q1-Q3) |
|
|
|
|
| CCI |
|
|||
| Mean±S.D |
|
|
|
|
| Median (Q1-Q3) |
|
|
|
|
| Anesthesia type |
|
|||
| Spinal |
|
|
|
|
| Spinal+Epidural |
|
|
|
|
| General |
|
|
|
|
| Hemoglobin (g/dL) |
|
|||
| Mean±S.D |
|
|
|
|
| Median (Q1-Q3) |
|
|
|
|
| Albumin (g/dL) |
|
|||
| Mean±S.D |
|
|
|
|
| Median (Q1-Q3) |
|
|
|
|
| Length of stay in SICU (days) |
|
|
||
| Mean±S.D |
|
|
|
|
| Median (Q1-Q3) |
|
|
|
|
| Length of stay in hospital (days) |
|
|||
| Mean±S.D |
|
|
|
|
| Median (Q1-Q3) |
|
|
|
|
The most common comorbidities were hypertension in 67.9% (n=93) of the entire population, CVD/HF in 34.3% (n=47), and diabetes in 29.9% (n=41). In the mortality group, only CVD/HF (61.1% vs. 30.2%, p=0.010) was significantly higher than in the survivor group (Table 2).
| CVD/HF: Coronary vascular disease/heart failure, COPD: Chronic obstructive pulmonary Disease. | ||||
| Table 2. Comorbidities in geriatric hip fracture patients. | ||||
| Comorbidity, n (%) |
|
|
|
|
| Hypertension |
|
|
|
|
| CVD/HF |
|
|
|
|
| Diabetes |
|
|
|
|
| Stroke |
|
|
|
|
| Asthma /COPD |
|
|
|
|
| Chronic renal failure |
|
|
|
|
After univariate analysis, multivariate analysis was performed. The risk ratio and 95% confidence interval were reported for each significant variable in multivariate analysis. ASA, APACHE-II, CCI, and GKS scores were found to be independent predictors of mortality (p=0.002, p=0.022, p=0.034, and p=0.002, respectively) (Table 3).
| ASA: American society of anesthesiologist, APACHE-II: Acute Physiology and Chronic Health Assessment-II, CCI: Charlson Comorbidity Index, GCS: Glasgow coma scale, CVD/HF: Coronary vascular disease/heart failure. | |||
| Table 3. Multivariate logistic regression analysis. | |||
|
|
|
|
|
| ASA status |
|
|
|
| APACHE-II |
|
|
|
| CCI |
|
|
|
| GCS |
|
|
|
| Albumin |
|
|
|
| CVD/HF |
|
|
|
When the prognostic values of the scores in predicting mortality were evaluated with ROC curve analysis, the cut-off value of the ASA score was ≥ 3.5, and the area under the curve (AUC) = 0.614 (95% CI, 0.458-0.769). The cut-off value of the APACHE-II score was ≥ 17.5 and AUC= 0.803 (95% CI, 0.697-0.908), and the cut-off value of CCI was ≥ 6.5 and AUC= 0.742 (95% CI, 0.598-0.886). The mortality prediction performances were determined based on the APACHE-II score, CCI, and ASA status, from highest to lowest. (Figure 2, Table 4).
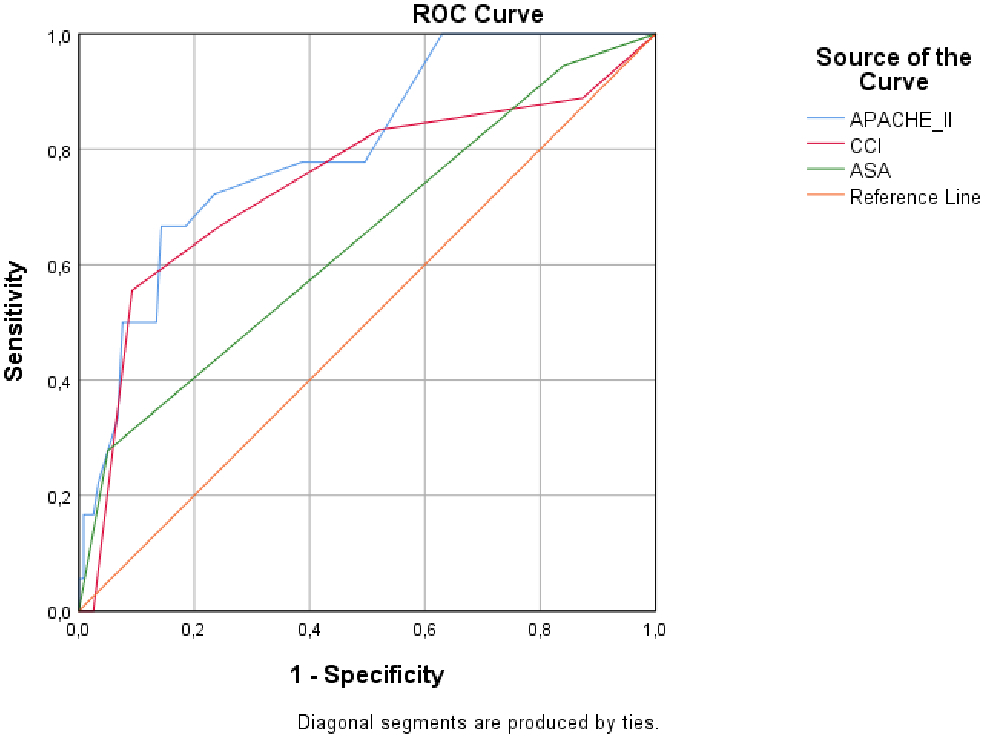
AUC: area under the curve, CI: confidence intervals, APACHE-II: Acute Physiology and Chronic Health Assessment-II, CCI: Charlson Comorbidity Index, ASA: American society of Anesthesiologist
| AUC: Area Under Curve, CI: Confidence interval, ASA: American society of anesthesiologist, APACHE-II: Acute Physiology and Chronic Health Assessment-II, CCI: Charlson Comorbidity Index, | ||||
| Table 4. Mortality prediction performance of ASA status, APACHE-II and CCI score. | ||||
|
|
|
|
|
|
| ASA status |
|
|
|
|
| APACHE-II |
|
|
|
|
| CCI |
|
|
|
|
Discussion
In this study conducted in a tertiary healthcare institution, low GCS scores, high ASA status and APACHE-II scores, and CCI were found to be associated with mortality in patients who underwent surgery due to geriatric hip fracture and were followed up in the SICU in the postoperative period. Comorbid diseases were not independent predictors of mortality. ASA status, APACHE-II, CCI, and GCS were determined to be independent predictors of mortality. In patients with geriatric hip fracture, the scores that performed best in predicting in-hospital mortality were APACHE-II (AUC=0.803), CCI (0.742), and ASA status (0.614), from highest to lowest.
Low-energy traumas, such as falls from the same level, are frequently seen in the geriatric population and mostly cause hip fractures (proximal femur fractures) (11). Approximately 30% of adults aged 60 and over fall annually (12). It has been reported that more than 1.5 million people are affected by hip fractures globally each year and that the highest mortality is seen within the first 30 days (13). Many parameters, such as type of injury, type of operation and surgical technique, early postoperative mobilization, postoperative cognitive impairment, and delirium, are associated with morbidity and mortality in the geriatric population. A meta-analysis reported that the female gender ratio was higher than male in patients with hip fractures and was determined as 61%-87.7% (14). Although it was reported that mortality was significantly higher in males, there are also studies reporting that gender does not affect mortality (15,16). The in-hospital mortality rate for geriatric hip fractures has been reported to be between 4-12% (17). It has been stated that the mortality risk is highest in the first 4 weeks after the fracture (15). In another study, it was stated that the in-hospital mortality rate for geriatric hip fractures was determined to be 32%. The authors reported that the high mortality rate may be due to the study’s inclusion of COVID-19-positive patients (18). In the current study, the in-hospital mortality rate in geriatric hip fractures was found to be 13.1%. Although the female gender ratio was high in the literature, gender did not significantly affect in-hospital mortality.
Various comorbidities such as hypertension, coronary artery disease, and diabetes are frequently encountered in the geriatric population. Increased comorbidities increase perioperative morbidity and mortality. Previous myocardial infarction and congestive heart failure have been reported to be predictors of mortality in the geriatric population (19). The ASA Physical Status Classification System classifies patients into six classes based on their current health status, including underlying medical conditions that may affect anesthesia. Patients with higher ASA status are associated with increased perioperative complications and mortality. Similarly, higher CCI scores have been associated with short- and long-term mortality in patients with hip fractures. (19,20). Haugan et al. reported that CCI and ASA scores have similar prognostic value in predicting mortality in patients with geriatric hip fractures (20). Hasan et al. found that the risk of developing postoperative complications in patients with high CCI scores was 1.45 times higher than in patients with low CCI scores (15). The authors also reported that the probability of developing postoperative complications in patients with higher ASA status was 1.77 times higher than in patients with low ASA status. Lakomkin et al. examined the relationship between CCI and postoperative side effects in repeat hip surgery. They stated that high CCI scores were associated with major complications. The authors also reported that CCI was significantly associated with mortality after surgery (21). In our study, coronary vascular disease/heart failure was found to be significantly higher in the mortality group. However, multivariate regression analysis determined that it was not an independent predictor of mortality. In addition, high ASA status and CCI were found to be independent predictors of mortality in hip fracture patients in the postoperative SICU. The predictive performance of CCI (>6) was found to be superior to the ASA score (>3) in predicting in-hospital mortality (AUC 0.742 vs. 0.614). However, complications other than in-hospital mortality were not evaluated in our study. CCI score provides more detailed scoring than the ASA classification. Health status and lifestyle factors such as smoking and obesity may be associated with mortality. However, they are not taken into account in CCI, while they are taken into account in ASA status. Accurate calculation of CCI score requires a comprehensive review of medical records. However, the superiority of CCI over ASA is more helpful in predicting in-hospital mortality.
The APACHE II score is a widely used, reliable, and easily administered tool for predicting mortality risk in patients monitored in the ICU based on their physiological values in the first 24 hours. The APACHE-II score evaluates 12 physiological parameters, as well as the patient’s age and previous health status. The maximum score is 71, with higher scores indicating a poor prognosis. The APACHE-II score is not a trauma-specific scoring system. It has been reported to be prognostic in predicting mortality in various patient groups monitored in the ICU. Furthermore, it has also been reported to help determine the prognosis in trauma patients (22-24). To our knowledge, the predictive performance of APACHE-II, which is routinely recorded in postoperative hip fracture patients followed in SICU, and CCI and ASA status in predicting mortality has not been compared. In our study, the predictive performance of the APACHE-II score was superior to both CCI and ASA status. The detailed structure of the APACHE-II score, which includes 12 physiological parameters, patient age, and surgical history, effectively prevented this situation from arising. However, CCI also has an acceptable prognostic value.
Other surgical and anesthesia-related conditions may affect mortality in patients with hip fractures. Some opinions state that the type of anesthesia does not affect mortality (4,18,25). In our study, however, it was determined that the type of anesthesia did not affect in-hospital mortality. Although it has been reported that the time from the fracture to the operation also affects mortality in hip fractures, there is no generally accepted opinion. It has been stated that in-hospital mortality increases in cases where the time from the fracture to the operation is more than 48 hours (26). Another study reported that delaying hip fracture surgery for up to four days did not increase mortality; however, mortality increased significantly with a delay of more than four days (27). In the current study, the time between the onset of hip fractures and the time until surgery was not evaluated because we did not have reliable data on this subject.
Malnutrition is common in geriatric patients with hip fractures. Malnutrition has been reported to increase comorbidities, increase healthcare costs, and lead to increased mortality rates (28). Serum albumin levels are used to determine malnutrition in the geriatric population. Albumin, a negative atrial phase protein, has been reported to help predict mortality in patients with traumatic brain injury and polytrauma (29). The prognostic nutritional index (PNI) is a marker derived from serum albumin levels. It has been reported to have prognostic value in geriatric hip fracture patients. Both PNI and CCI have been reported in the literature to be independent predictors of mortality in geriatric patients with hip fractures (30). In the current study, serum albumin levels at the time of SICU admission were significantly lower in the mortality group. However, hypoalbuminemia was not found to be an independent predictor of mortality. Since the aim of the study was not to determine the prognostic value of PNI, it was not evaluated.
Study limitations
The study has several limitations. First, it is a retrospective observational study. Second, it included patients with critical hip fractures from a single institution. This may make it difficult to generalize the results to a larger population. Third, in-hospital mortality was the primary outcome of the study. Long-term mortality was not assessed. Furthermore, the mortality group consisted of a small number of patients (n=18). The small size of the mortality group may have affected the validity of the ROC analyses. Fourth, the time to surgery in patients with hip fractures is crucial for both morbidity and mortality. We were unable to assess this timeframe in the current study because we did not have access to these specific timeframes. Fifth, complications that occurred during the patients’ SICU follow-up were not evaluated.
Conclusion
In conclusion, hip fractures resulting from low-energy trauma in the geriatric population are significant causes of morbidity and mortality. CCI, ASA status, and APACHE-II score were found to be independent predictors of mortality in critically ill geriatric patients with frequent comorbidities. The prognostic values of the scores in in-hospital mortality are listed from highest to lowest according to APACHE-II, CCI, and ASA status. All three scores have acceptable prognostic value in identifying critically ill patients within the first month when mortality rates are high in critical geriatric hip fracture patients.
Ethical approval
This study has been approved by the University of Health Sciences, Istanbul Kanuni Sultan Süleyman Training and Research Hospital Clinical Trials Review Board and Ethics Committee (approval date: 08.05.2024, number: KAEK/2024.05.89). Written informed consent was obtained from the participants.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- McDonough CM, Harris-Hayes M, Kristensen MT, et al. Physical therapy management of older adults with hip fracture. J Orthop Sports Phys Ther. 2021;51:CPG1-CPG81. https://doi.org/10.2519/jospt.2021.0301
- T.C. İçişleri Bakanlığı, Nüfus ve Vatandaşlık İşleri Genel Müdürlüğü. Türkiye İstatistik Kurumu Haber Bülteni. 2023. Available at: https://data.tuik.gov.tr/Bulten/Index?p=Adrese-Dayali-Nufus-Kayit-Sistemi-Sonuclari-2023-49684 (Accessed on Dec 30, 2024).
- Kirshenbom D, Ben-Zaken Z, Albilya N, Niyibizi E, Bala M. Older age, comorbid illnesses, and injury severity affect immediate outcome in elderly trauma patients. J Emerg Trauma Shock. 2017;10:146-50. https://doi.org/10.4103/JETS.JETS_62_16
- Arslan K, Celik S, Arslan HC, Sahin AS, Genc Y, Erturk C. Predictive value of prognostic nutritional index on postoperative intensive care requirement and mortality in geriatric hip fracture patients. North Clin Istanb. 2024;11:249-57. https://doi.org/10.14744/nci.2024.60430
- Clare D, Zink KL. Geriatric trauma. Emerg Med Clin North Am. 2021;39:257-71. https://doi.org/10.1016/j.emc.2021.01.002
- Arslan K, Şahin AS, Yalçın N, Kaya E. Evaluation of trauma patients followed up and treated in intensive care unit: the sample of İstanbul province training and research hospital. Turk J Intensive Care. 2023;21:41-7. https://doi.org/10.4274/tybd.galenos.2022.20591
- Haywood KL, Brett J, Tutton E, Staniszewska S. Patient-reported outcome measures in older people with hip fracture: a systematic review of quality and acceptability. Qual Life Res. 2017;26:799-812. https://doi.org/10.1007/s11136-016-1424-1
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-83. https://doi.org/10.1016/0021-9681(87)90171-8
- Varady NH, Gillinov SM, Yeung CM, Rudisill SS, Chen AF. The charlson and elixhauser scores outperform the American society of anesthesiologists score in assessing 1-year mortality risk after hip fracture surgery. Clin Orthop Relat Res. 2021;479:1970-9. https://doi.org/10.1097/CORR.0000000000001772
- Baykan N, Durukan P, Salt O, et al. Examination of geriatric trauma patients presenting to the emergency department. Phnx Med J. 2022;4:22-6. https://doi.org/10.38175/phnx.1037855
- Montero-Odasso MM, Kamkar N, Pieruccini-Faria F, et al. Evaluation of clinical practice guidelines on fall prevention and management for older adults: a systematic review. JAMA Netw Open. 2021;4:e2138911.
- Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int. 2009;20:1633-50. https://doi.org/10.1007/s00198-009-0920-3
- Hu F, Jiang C, Shen J, Tang P, Wang Y. Preoperative predictors for mortality following hip fracture surgery: a systematic review and meta-analysis. Injury. 2012;43:676-85. https://doi.org/10.1016/j.injury.2011.05.017
- Schousboe JT. Mortality after osteoporotic fractures: what proportion is caused by fracture and is preventable? J Bone Miner Res. 2017;32:1783-8. https://doi.org/10.1002/jbmr.3216
- Hasan O, Barkat R, Rabbani A, Rabbani U, Mahmood F, Noordin S. Charlson comorbidity index predicts postoperative complications in surgically treated hip fracture patients in a tertiary care hospital: retrospective cohort of 1045 patients. Int J Surg. 2020;82:116-20. https://doi.org/10.1016/j.ijsu.2020.08.017
- Frost SA, Nguyen ND, Black DA, Eisman JA, Nguyen TV. Risk factors for in-hospital post-hip fracture mortality. Bone. 2011;49:553-8. https://doi.org/10.1016/j.bone.2011.06.002
- Kılınç G, Karakuş Ö, Gürer B. The role of ASA score and Charlson comorbidity index in predicting in-hospital mortality in geriatric hip fracture patients. Eur Rev Med Pharmacol Sci. 2023;27:7065-72.
- Karres J, Kieviet N, Eerenberg JP, Vrouenraets BC. Predicting early mortality after hip fracture surgery: the hip fracture estimator of mortality Amsterdam. J Orthop Trauma. 2018;32:27-33. https://doi.org/10.1097/BOT.0000000000001025
- Lau T, Fang C, Fang C, Leung F. Assessment of postoperative short-term and long-term mortality risk in Chinese geriatric patients for hip fracture using the Charlson comorbidity score. Hong Kong Med J. 2016;22:16-22.
- Haugan K, Klaksvik J, Foss OA. 30-day mortality in patients after hip fracture surgery: a comparison of the Charlson comorbidity index score and ASA score used in two prediction models. Injury. 2021;52:2379-83. https://doi.org/10.1016/j.injury.2021.02.004
- Lakomkin N, Goz V, Lajam CM, Iorio R, Bosco JA. Higher modified Charlson index scores are associated with increased incidence of complications, transfusion events, and length of stay following revision hip arthroplasty. J Arthroplasty. 2017;32:1121-24. https://doi.org/10.1016/j.arth.2016.11.014
- Arslan K, Arslan HÇ, Şahin AS. Evaluation of critically ill obstetric patients treated in an intensive care unit during the COVID-19 pandemic. Ann Saudi Med. 2023;43:10-6. https://doi.org/10.5144/0256-4947.2023.10
- Sungurtekin H, Sargın F, Kılınç M, et al. Usefulness of APACHE-II, SOFA, ISARIC/WHO 4C Mortality Score and CO-RADS for mortality prediction of critically Ill Coronavirus Disease-2019 patients. Turk J Intensive Care. 2023;21:100-9. https://doi.org/10.4274/tybd.galenos.2022.77598
- Arslan K, Sahin AS. Prognostic value of systemic immune-inflammation index, neutrophil-lymphocyte ratio, and thrombocyte-lymphocyte ratio in critically ill patients with moderate to severe traumatic brain injury. Medicine (Baltimore). 2024;103:e39007. https://doi.org/10.1097/MD.0000000000039007
- Kunutsor SK, Hamal PB, Tomassini S, Yeung J, Whitehouse MR, Matharu GS. Clinical effectiveness and safety of spinal anaesthesia compared with general anaesthesia in patients undergoing hip fracture surgery using a consensus-based core outcome set and patient-and public-informed outcomes: a systematic review and meta-analysis of randomised controlled trials. Br J Anaesth. 2022;129:788-800. https://doi.org/10.1016/j.bja.2022.07.031
- Ram GG, Govardhan P. In-hospital mortality following proximal femur fractures in elderly population. Surg J (N Y). 2019;5:e53-6. https://doi.org/10.1055/s-0039-1692995
- Moran CG, Wenn RT, Sikand M, Taylor AM. Early mortality after hip fracture: is delay before surgery important? J Bone Joint Surg Am. 2005;87:483-9. https://doi.org/10.2106/JBJS.D.01796
- Soukkio P, Suikkanen S, Kääriä S, et al. Effects of 12-month home-based physiotherapy on duration of living at home and functional capacity among older persons with signs of frailty or with a recent hip fracture - protocol of a randomized controlled trial (HIPFRA study). BMC Geriatr. 2018;18:232. https://doi.org/10.1186/s12877-018-0916-y
- Arslan K, Sultan Sahin A. Lactate, lactate clearance, and lactate-to-albumin ratio in predicting mortality in patients with critical polytrauma: a retrospective observational study. Medicine (Baltimore). 2024;103:e40704. https://doi.org/10.1097/MD.0000000000040704
- Feng L, Fu S, Yao Y, Yuan W, Zhao Y. Age, prognostic nutritional index, and charlson comorbidity index were independent risk factors for postoperative long-term mortality in Chinese geriatric patients who sustain hip fracture. J Am Med Dir Assoc. 2021;22:2602-3. https://doi.org/10.1016/j.jamda.2021.08.001
Copyright and license
Copyright © 2025 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.









