Abstract
Objective: To synthesize current evidence on the integration of palliative care into the care of critically ill patients, with a focus on models of delivery, symptom management, communication frameworks, ethical dimensions, and emerging trends in the field.
Materials and Methods: This narrative review was conducted through a structured literature search of PubMed, MEDLINE, and Cochrane databases using terms including ‘palliative care,’ ‘intensive care unit,’ ‘critical illness,’ ‘goals of care,’ and ‘symptom management,’ restricted to English-language articles published between 2000 and 2024. Articles were selected based on relevance to the review’s core domains and methodological quality, prioritizing randomized controlled trials, systematic reviews, and consensus guidelines where available.
Results: Early and structured integration of palliative care in the ICU is associated with improved symptom control, reduced rates of post-intensive care syndrome in patients and families, decreased non-beneficial interventions, shorter ICU stays at end of life, and lower healthcare costs without increasing mortality. Structured communication interventions and validated trigger-based referral criteria demonstrate consistent benefit. Evidence is strongest in medical ICU and oncology populations; emerging data support application across neurocritical care, cardiac, and surgical ICUs.
Conclusion: As ICU populations continue to age and life-sustaining treatments grow more complex, integrating palliative care principles alongside intensive therapies is essential to providing high-quality, goal-concordant, and compassionate critical care globally.
Keywords: palliative care, intensive care unit, critical illness, goals of care, shared decision-making, symptom management, neurocritical care, cardiac intensive care, post-intensive care syndrome, end-of-life care
Introduction
Each year, between 5 and 6 million patients are admitted to ICUs in the United States alone, and in high-income countries an estimated 10-20% of all deaths occur in or shortly after an ICU stay (1,2). For many of these patients, the course of illness is neither brief nor predictable. They arrive in crisis, stabilize, deteriorate again, and may spend days or weeks in a state of profound physiological and existential uncertainty, sustained by technology, unable to communicate, dependent on surrogates who are themselves navigating grief and unfamiliar decisions (1,2). Technical excellence in organ support is necessary, but it is not enough. Meeting the full range of needs generated by critical illness requires something more: a parallel commitment to understanding what patients value, relieving what they suffer, and ensuring that the care delivered also reflects who they are, not only what their physiology demanded.
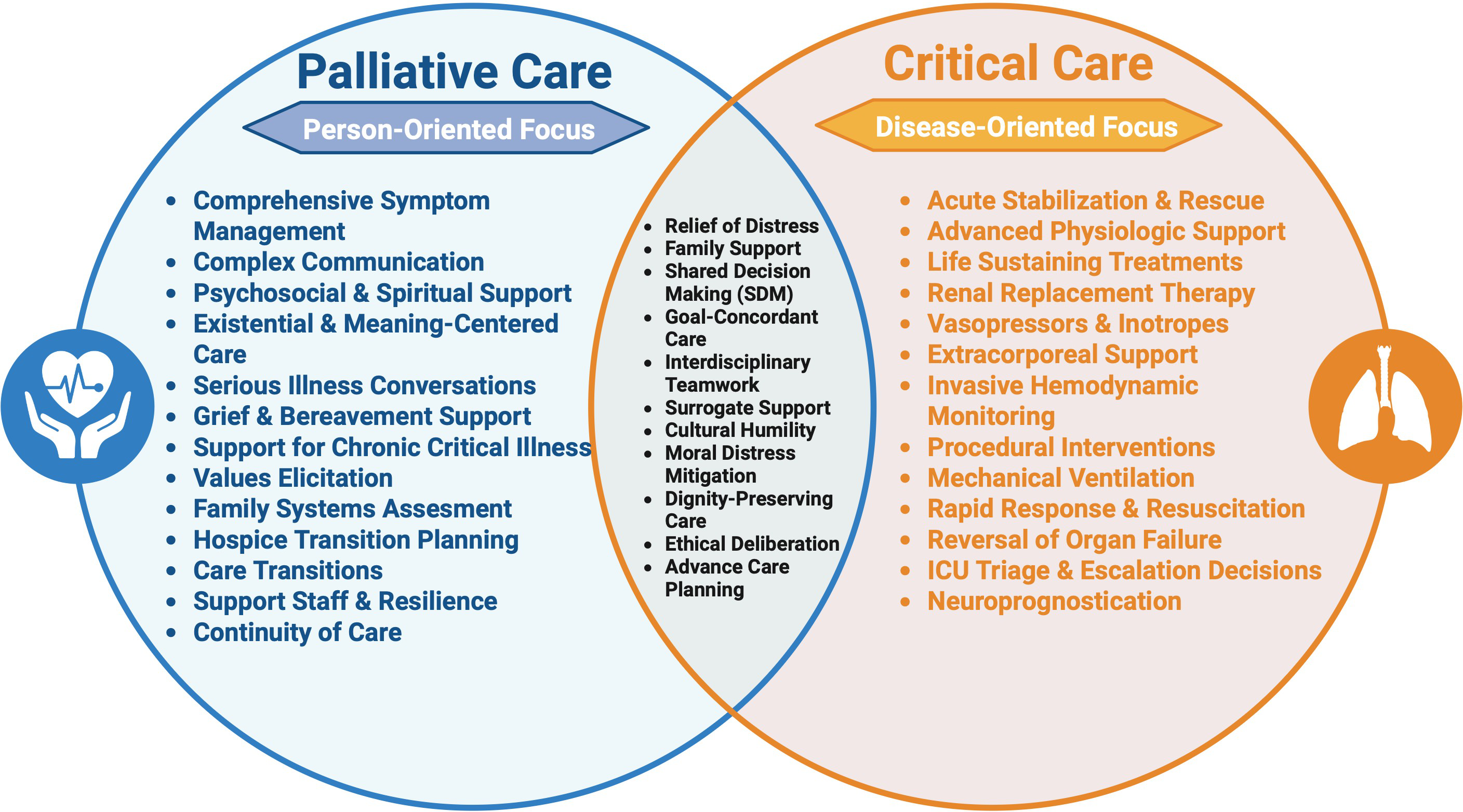
Palliative care is specialized clinical care focused on improving quality of life for patients with serious illness and their families and care partners, delivered by a multidisciplinary team through symptom management, communication, and support for shared decision-making (3). Importantly, palliative care is not synonymous with hospice or end-of-life care; it is appropriate at any stage of serious illness and is designed to be delivered alongside curative or life-prolonging therapies. The World Health Organization (WHO) defines palliative care as an approach that “affirms life and regards dying as a normal process,” neither hastening nor postponing death, and calls for its integration across all levels of the health system, including critical care (4,5) (Figure 1).
The need for this review is both clinical and contextual. While much of the foundational evidence for ICU palliative care integration has emerged from the United States, Canada, and Western Europe, settings with well-resourced palliative care infrastructure, specialist workforce pipelines, and specific insurance-based referral structures, the principles and evidence are increasingly relevant to health systems worldwide. In the Eastern Mediterranean and Middle Eastern region, palliative care programs are in varying stages of development, and intensivists often serve as the primary or sole providers of palliative support for critically ill patients (4,6). The integration models and communication frameworks discussed in this review must therefore be interpreted and adapted to local healthcare structures, cultural values, and available resources. Where possible, we highlight evidence that spans diverse healthcare contexts.
This narrative review synthesizes current evidence on the role of palliative care across ICU settings, focusing on the medical ICU (MICU), neurocritical care unit (NCCU), and cardiac ICU (CICU) as settings with distinct patient populations and palliative care demands. We examine models of integration, symptom management, serious illness communication, ethical dimensions, and emerging directions, with the goal of providing a practical and evidence-based framework for clinicians working in any critical care environment. While palliative care needs have grown across all ICU settings as patient populations age and treatment complexity increases, this review focuses specifically on three settings where the evidence base and clinical demands are particularly distinct: the MICU, the NCCU, and the CICU.
Defining palliative care in the ICU context
Critically-ill patients experience a profound and often underappreciated symptom burden. Studies using systematic assessment tools in ICU populations have documented that more than 50% of patients who are mechanically ventilated or have altered consciousness experience moderate-to-severe pain, and that dyspnea, anxiety, and agitation are present in the majority of patients at some point during their admission (7). Delirium affects 60-80% of patients who are mechanically ventilated and is independently associated with increased mortality, prolonged ICU stay, and long-term cognitive impairment (8,9). These symptoms are frequently undertreated, in part because patients are non-communicative and standard self-report instruments cannot be used.
What makes the ICU a distinct palliative care environment is not simply that patients are seriously ill - that is true in many settings. It is the convergence of features that defines the critical care context: patients are often unable to speak, so their suffering must be inferred and their values reconstructed from the people who love them. Families arrive in a state of shock, frequently without any prior conversation about what their loved one would want. Decisions that carry permanent consequences, whether to pursue tracheostomy, whether to continue mechanical ventilation, whether to withdraw life support, must sometimes be made within days or even hours, before anyone has had time to absorb what has happened. And clinicians are often simultaneously managing physiological crises and navigating the most important conversations of a family’s life. Prognostic uncertainty exists across many serious illnesses, but in the ICU it lands differently: not as something to sit with over months of outpatient visits, but as something to act on now.
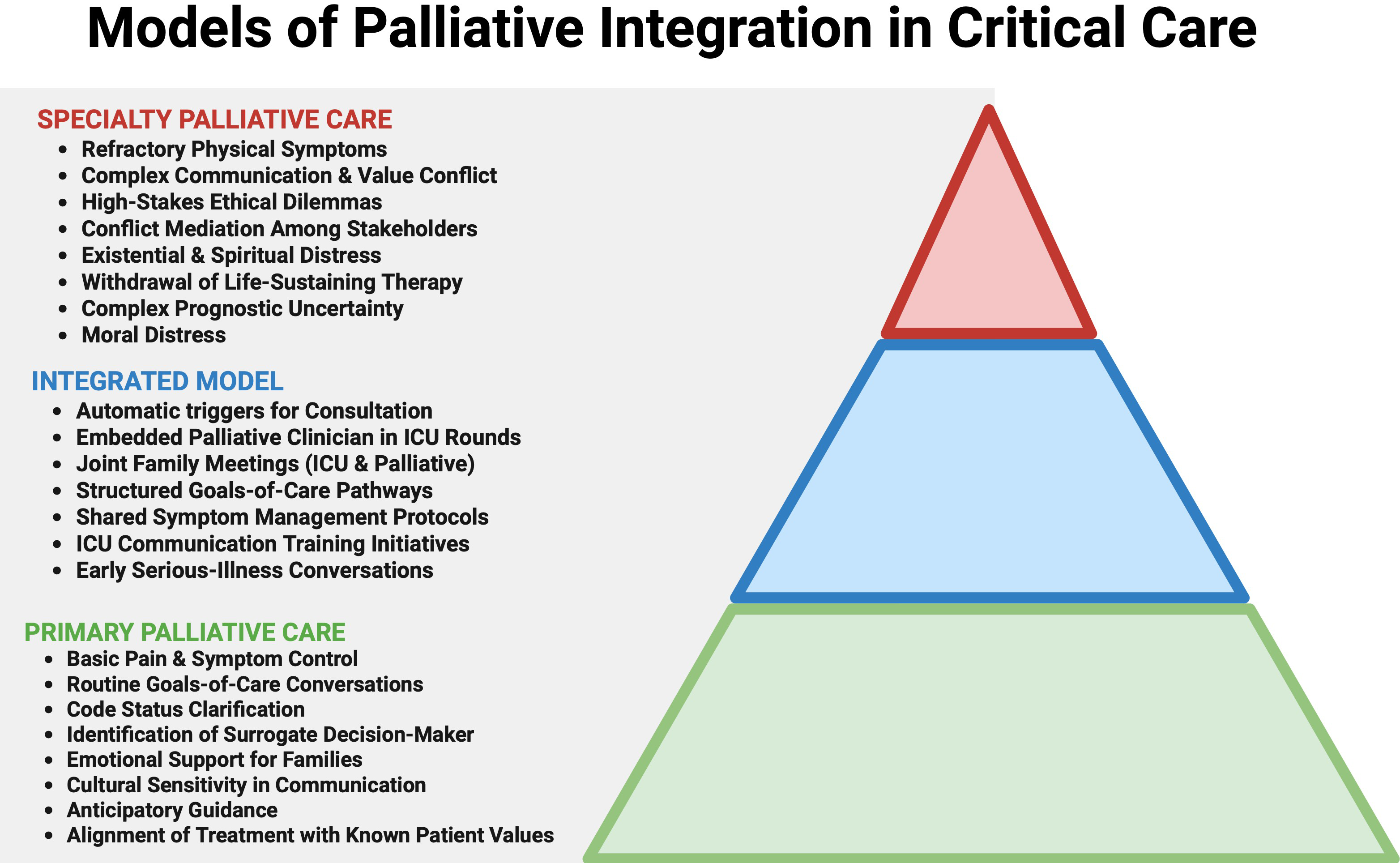
Three models of palliative care delivery have been described and studied in the ICU setting, and understanding the distinctions between them matters practically, because the right model for a given patient, clinician, or institution depends heavily on context (10). In the primary palliative care model, basic symptom assessment, comfort-focused care, and goals-of-care conversations are conducted by the ICU team itself. This is not a lesser form of palliative care; it is the foundation upon which specialist involvement builds, and in much of the world it represents the only palliative care critically ill patients will receive. In the integrated model, specialist palliative care clinicians work alongside ICU teams in a sustained, longitudinal way, attending rounds, co-facilitating family meetings, and providing continuity across a patient’s ICU stay. In the consultative model, specialist teams are called upon for the most complex situations: refractory symptoms, protracted family conflict, requests to withdraw life-sustaining therapies, or ethical disputes that the primary team cannot resolve alone. These models are not mutually exclusive, and in the best-resourced settings they operate in concert. But even where specialist palliative care is limited, a primary care model grounded in communication skills and symptom awareness can meaningfully improve the experience of critically ill patients and their families (Figure 2).
Palliative care across ICU settings
The medical ICU (MICU)
The MICU has been the primary setting for palliative care integration research, and the evidence base here is the most robust. Patients admitted to the MICU frequently carry diagnoses of advanced malignancy, decompensated heart failure, respiratory failure, or sepsis, conditions with high short-term mortality, substantial symptom burden, and clinical trajectories that often shift rapidly toward end of life during the hospitalization itself.
Structured family meeting interventions have demonstrated the clearest and most consistent benefits in this population. The randomized trial by Carson and colleagues found that palliative care-led family meetings for patients with chronic critical illness significantly improved family members’ emotional outcomes and reduced symptoms of PTSD at 90 days compared to usual care (11). Lilly and colleagues demonstrated in a prospective cohort study that a mandatory communication intervention in the MICU, consisting of structured family meetings within 72 hours of admission and palliative care involvement for high-risk patients, reduced ICU length of stay by more than 30% among patients who ultimately died, without increasing overall mortality (12). A systematic review by Khandelwal and colleagues similarly found that palliative care interventions and advance care planning in the ICU were associated with reductions in ICU length of stay for patients who died, again without increasing mortality, a finding that directly addresses the common concern that palliative involvement hastens death (13).
What makes the MICU population particularly distinct from a palliative care standpoint is the frequency with which patients arrive having never had a serious illness conversation, and the speed with which their condition can deteriorate to a point where those conversations become urgent. Many MICU patients are admitted with diagnoses that carry a high likelihood of in-hospital death, septic shock, acute respiratory failure, multi-organ failure, yet arrive without documented advance directives and with families who have had no opportunity to prepare. The palliative care imperative in the MICU is therefore one of compression: the work that ideally happens over months of outpatient serious illness conversations must be accomplished in days, in a family that is simultaneously in crisis. Trigger-based referral models, proactive family meetings, and structured communication frameworks are not supplementary to MICU care in this context, they are essential to ensuring that the care delivered in the final days of a patient’s life reflects who that patient was, not simply what their physiology allowed.
The neurocritical care unit (NCCU)
Palliative care in the NCCU presents a distinct set of challenges that merit particular attention. Patients admitted with devastating neurological injuries including severe traumatic brain injury, malignant hemispheric stroke, subarachnoid hemorrhage, or hypoxic-ischemic encephalopathy following cardiac arrest, face a clinical landscape defined not simply by prognostic uncertainty, but by the need to navigate irreversible, time-sensitive decisions in the absence of reliable long-term prognostic data.
Families in the NCCU are frequently under pressure, from the pace of the ICU environment, from uncertainty about what to hope for, and sometimes from clinical teams themselves, to make decisions about goals of care before reliable prognostic information is available. Current best practice in neurocritical care strongly cautions against early prognostication and early withdrawal decisions in the acute phase, recognizing that neurological recovery trajectories can be profoundly unpredictable in the first days following injury (14). The role of palliative care in the NCCU is therefore not to facilitate early decisions, but to help families and clinicians resist premature closure, holding space for uncertainty, clarifying patient values, and ensuring that any decisions made are anchored in what is known rather than what is feared. There is well-documented risk of premature mortality secondary to early withdrawal of life-sustaining treatment in this setting, often driven by pessimistic prognostication that does not account for the brain’s capacity for recovery (14). Structured palliative involvement serves as a safeguard against this risk by centering patient values rather than clinician prognostic uncertainty in the decision-making process.
The integration of palliative care in the NCCU has been associated with improved documentation of goals of care, earlier clarification of treatment preferences, and a reduction in non-beneficial interventions at the end of life (15,16). Communication frameworks adapted to the NCCU context, emphasizing honest acknowledgment of uncertainty, the importance of patient values in guiding decisions, and the option to revisit initial decisions as the clinical picture evolves, are core to high-quality care in this setting.
What makes the NCCU population uniquely challenging from a palliative care standpoint is the intersection of three features that rarely converge so acutely in other settings: neurological injuries that may render patients permanently unable to participate in their own care, prognostic uncertainty that is genuine and not merely a function of limited information, and a decision-making timeline that is compressed by the biology of acute brain injury. A family navigating a loved one’s devastating stroke is not simply dealing with a difficult prognosis, they are being asked to make irreversible decisions about a person whose neurological future cannot yet be known, often within days of an event that has upended everything they understood about that person’s life. Palliative care in the NCCU exists to ensure that those decisions, whenever they are made, are made well, with full understanding of the uncertainty, grounded in patient values, and with the emotional and informational support families need to carry them forward.
The cardiac ICU (CICU)
The CICU landscape has changed considerably over the past two decades. Where it once served primarily as a setting for managing acute myocardial infarction and arrhythmia, it now increasingly cares for patients with end-stage heart failure, cardiogenic shock, and complex structural disease, patients whose prognosis is often poor but whose trajectory is notoriously difficult to predict. Heart failure does not follow a clean downward decline; it moves in sudden drops and partial recoveries in ways that leave both clinicians and families uncertain about when, if ever, the time for comfort-focused care has arrived.
This prognostic complexity is compounded by the availability of mechanical cardiac support that can sustain life, sometimes indefinitely, without restoring meaningful function. A patient on veno-arterial extracorporeal membrane oxygenation (ECMO) or a durable left ventricular assist device may be alive in every measurable physiological sense while being unable to participate in any of the activities that gave their life meaning. Conversations about device deactivation are among the most ethically weighted in all of critical care: they require clinicians to navigate questions of medical futility, patient autonomy, and the moral status of devices that patients may experience as extensions of themselves (17). Palliative care teams bring specific expertise to these conversations, and their involvement has been associated with improved patient and family satisfaction and reduced decisional conflict (17). Equally important is attention to symptom burden: dyspnea in advanced heart failure can be severe and is frequently under-treated in settings where the clinical focus is procedural. Addressing it is not peripheral to CICU care. It is part of it.
What distinguishes the CICU population from a palliative care standpoint is the particular cruelty of heart failure’s trajectory combined with the false reassurance that mechanical support can create. Families of patients on ventricular assist devices or ECMO may believe, reasonably, that the presence of the technology means recovery remains possible, and clinicians in a procedurally oriented culture may be slow to initiate conversations that challenge that assumption. The result is that goals-of-care conversations in the CICU frequently happen too late, after patients have lost the capacity to participate in them, and after families have spent weeks or months emotionally committed to a trajectory of recovery that the clinical picture no longer supports (18). Palliative care integration in the CICU addresses this not by hastening difficult conversations, but by ensuring they happen while patients still have a voice, and by helping families understand that the question is not whether to fight for their loved one, but what their loved one would consider worth fighting for.
Symptom burden in the critically ill
One of the practical challenges of palliative care in the ICU is that the patients who most need symptom assessment are often those least able to report their symptoms. A patient on mechanical ventilation cannot say that she is in pain. A patient with delirium cannot reliably describe what he is experiencing. This is not a minor inconvenience, it is a fundamental clinical problem, and one that has driven the development of behavioral assessment tools specifically designed for the critical care environment. The Critical-Care Pain Observation Tool (CPOT) (19), the Richmond Agitation-Sedation Scale (RASS) (20), and the Confusion Assessment Method for the ICU (CAM-ICU) (21) represent validated, bedside-usable instruments that allow clinicians to systematically assess pain, sedation depth, and delirium in patients who cannot self-report (8). Embedded in the 2018 PADIS guidelines, these tools are now standard of care, but their consistent application in practice remains variable, and under-treatment of pain and delirium in the ICU remains a documented problem (8). Managing symptoms in the critically ill requires a different calculus than in other settings. Opioids, which carry well-founded concerns about respiratory depression in other contexts, are essential for managing dyspnea in patients transitioning to comfort-focused care, and evidence is clear that when appropriately titrated to symptom relief, they do not hasten death (8,22). Sedation must balance comfort against the cognitive costs of over-sedation. Delirium, which affects 60-80% of mechanically ventilated patients, demands non-pharmacological prevention strategies as a first line, reorientation, early mobility, sleep hygiene, because no pharmacological treatment has demonstrated reliable efficacy in reducing its incidence or duration (8). These are not straightforward clinical problems, and they require the kind of sustained, expert attention that palliative care teams are specifically trained to provide.
Beyond the patient, the symptom burden of critical illness extends to families and surrogate decision-makers. Up to 70% of family members of ICU patients experience clinically significant anxiety, and approximately one-third meet criteria for PTSD, depression, or complicated grief in the months following their loved one’s ICU stay, a phenomenon now formally recognized as post-intensive care syndrome-family (PICS-F) (23-27). Structured communication, proactive family meetings, and anticipatory guidance about what to expect during and after the ICU course are core palliative competencies that have been shown to reduce long-term psychological distress in surrogates (28). A randomized trial by Lautrette and colleagues demonstrated that a structured communication intervention, including a proactive family conference and a bereavement brochure, significantly reduced the proportion of family members who met PTSD criteria at 90 days following patient death in the ICU (28).
Ethical dimensions and health system outcomes
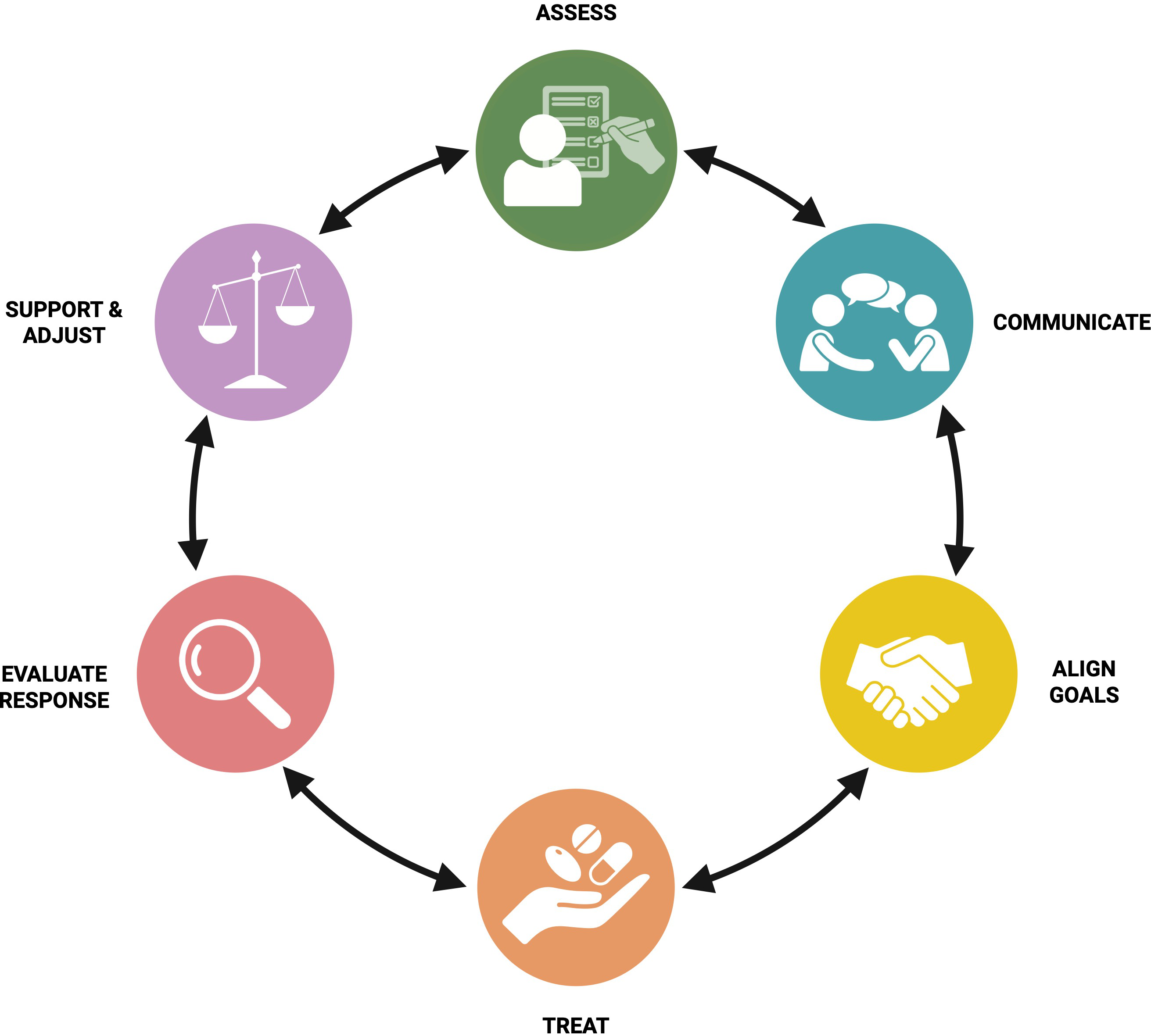
The ethical tensions that arise in the ICU are not abstract, they emerge from real clinical situations, often in the middle of the night, when a patient’s condition changes and the treatment path forward is no longer clear. Should a patient with severe hypoxic-ischemic encephalopathy receive a tracheostomy? Should ECMO be continued in a patient whose neurological injury now appears irreversible? When a surrogate’s decision seems inconsistent with what the patient once expressed, how should the clinical team respond? These are the questions in which palliative care teams do some of their most important work, not by overriding clinical judgment, but by creating the conditions under which good judgment can be exercised. The ethical framework underlying these conversations draws on principles of beneficence, non-maleficence, and autonomy, but these principles do not resolve ICU dilemmas by themselves (35,36). Beneficence in critical care requires asking not just ‘can we sustain this person’s life?’ but ‘does doing so serve their interests?’ Non-maleficence demands a frank accounting of what aggressive treatment actually costs a patient who may not be able to recover. Autonomy, frequently exercised through surrogates in the ICU, requires that clinicians actively support decision-makers in understanding their role, substituted judgment, not personal preference. Palliative care teams are trained to hold all three principles in tension simultaneously, and their involvement has been shown to reduce ethical conflicts, improve advance directive documentation, and support clinicians in delivering care that is both rigorous and humane (35) (Figure 3).
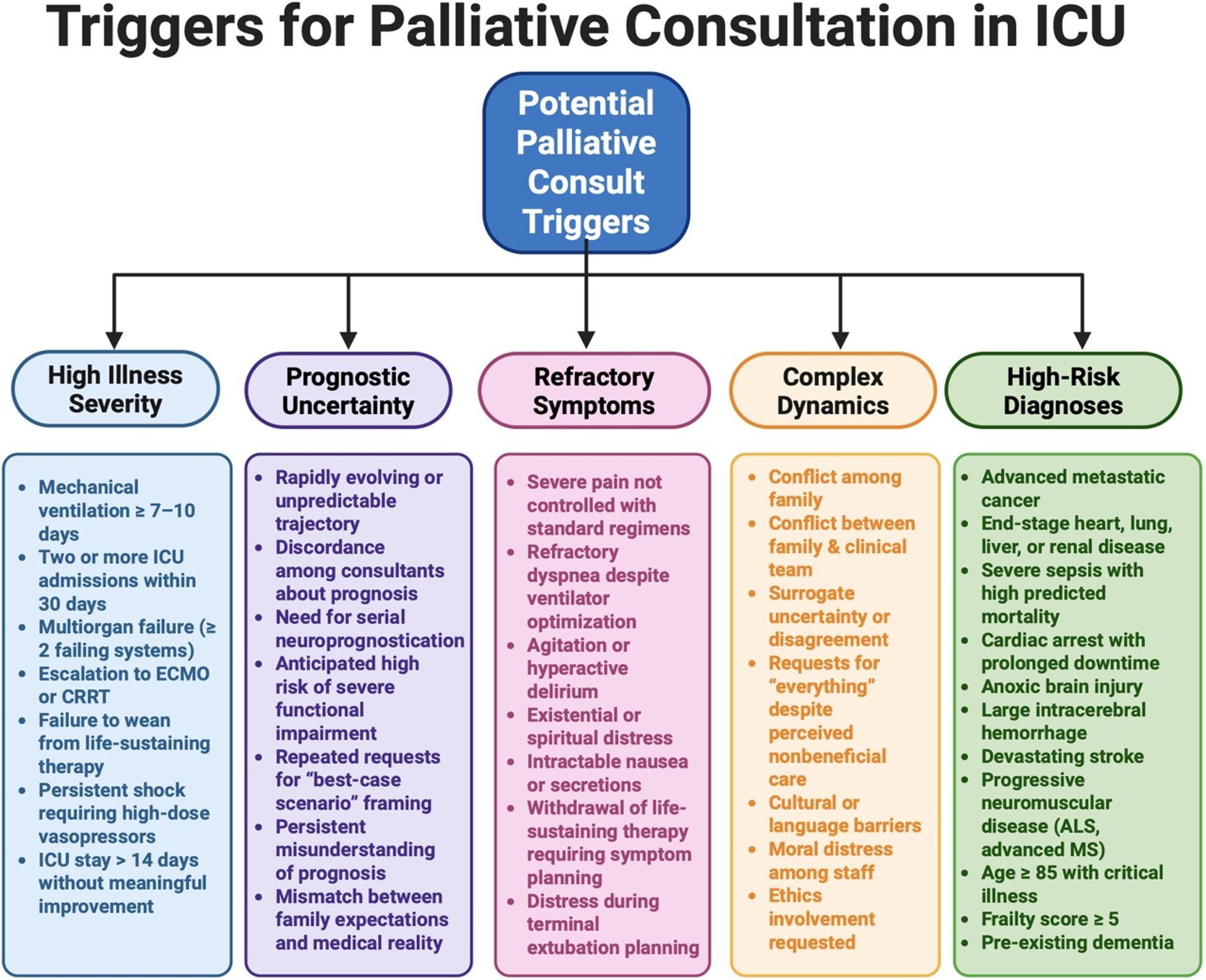
The health system effects of palliative care integration in the ICU are well-documented. Early palliative involvement is consistently associated with reduced non-beneficial interventions, shorter ICU stays among patients nearing the end of life, fewer invasive procedures, and lower overall healthcare costs without an increase in mortality (12,13,37). Penrod and colleagues demonstrated in a large observational study that hospital-based palliative care consultation was associated with significant reductions in hospital costs, particularly in patients with high illness severity (37). Evidence supports the use of trigger criteria, including ICU stay duration greater than seven days, advanced malignancy, severe neurological injury, dependence on mechanical ventilation, and multi-organ failure, to systematically identify patients who would benefit from palliative care involvement (38). Trigger-based consultation models have been implemented in multiple ICU settings and shown to improve the timeliness of goals-of-care conversations and reduce non-beneficial treatment at the end of life (10,38). It should be noted, however, that trigger criteria vary across institutions, are not universally validated, and should be adapted to local clinical context and institutional resources rather than applied prescriptively (Figure 4).
Emerging trends and future directions
Palliative care in the ICU is not a static field. Several developments in recent years are reshaping how it is delivered, who has access to it, and how clinicians are trained to provide it, and they are worth noting not as abstract trends but as practical opportunities. Tele-palliative care has moved from a pandemic-era adaptation to a recognized delivery model. Palliative consultations conducted via videoconference have shown acceptability to patients and families and outcomes comparable to in-person consultation, particularly for goals-of-care conversations that do not require physical examination (39). For ICUs in rural or community hospital settings, and for health systems in countries where specialist palliative care teams are concentrated in major academic centers, this represents a meaningful expansion of access to expertise that was previously unavailable (39).
Equity in palliative care access is increasingly recognized as an urgent problem. In the United States, Black and Hispanic patients are significantly less likely to receive palliative care consultation and less likely to have documented advance directives, even after controlling for disease severity and insurance status (40,41). The reasons are multiple, historical distrust of the medical system, communication barriers, implicit bias in referral patterns, and structural underrepresentation of diverse populations in the palliative care workforce. Addressing these gaps requires more than expanding the number of palliative care teams; it requires training clinicians in culturally responsive communication and ensuring that serious illness conversations are conducted in patients’ preferred languages with professional interpretation, not family members pressed into an impossible role.
Clinician training is evolving as well. Programs such as VitalTalk (42), the IPAL-ICU curriculum (43), and End-of-Life Nursing Education Consortium (ELNEC) critical care modules (44) have been developed and evaluated specifically for the ICU context. What they share is an emphasis on communication as a clinical skill, one that can be taught, practiced, and improved, rather than a personality trait that clinicians either possess or do not. This framing matters: it means that the quality of serious illness conversations in the ICU is not fixed, and that investment in training has measurable returns for patients and families.
Finally, artificial intelligence and machine learning models are being developed to identify, earlier and more accurately, which ICU patients are at highest risk of death or prolonged functional dependence. The goal is to enable earlier, more proactive palliative engagement, to trigger a goals-of-care conversation before a family is in crisis rather than after. This is genuinely promising. Despite this, it does carry a real risk: a risk that algorithmic prognostication will substitute for individualized clinical judgment, that families will receive predictions rather than conversations, and that the quantification of prognosis will crowd out the human work of helping patients and families understand what the numbers mean for them. Used well, these tools can serve to extend clinical reach. However used poorly, they can reduce it.
Limitations
As a narrative review, the selection of literature reflects the authors’ clinical expertise and is not exhaustive; findings should be interpreted with the understanding that this methodology carries an inherent risk of selection bias and does not capture the totality of available evidence.
Several additional limitations merit acknowledgment. First, the evidence base synthesized in this review is heavily weighted toward studies conducted in the United States, Canada, and Western Europe, where palliative care infrastructure, specialist workforce availability, and insurance-based referral structures may differ from other regions, and findings should therefore be adapted rather than directly applied to these contexts. Second, while this review addresses palliative care across the MICU, NCCU, and CICU, the evidence is uneven across settings, conclusions are strongest for medical ICU populations, and more high-quality research is needed in neurocritical and cardiac care environments before equivalent recommendations can be made. Third, several of the landmark trials informing this review were conducted 15-25 years ago, and advances in ICU technology, staffing models, and standard of care since that time may limit the direct applicability of their findings to contemporary critical care practice. Finally, as with any clinical literature, publication bias may have resulted in an overrepresentation of positive findings, and the true effect of palliative care integration across all ICU contexts may be more modest than the available evidence suggests.
Conclusion
Palliative care is not the endpoint of critical care, it is woven into its fabric. From the moment a patient arrives in the ICU, the questions that palliative care is designed to address are already present: What symptoms is this person experiencing? What do they value? What would patients want if they could speak for themselves? What do their family members and surrogate decision-makers need to navigate this crisis? The evidence reviewed here demonstrates consistently that structured, early integration of palliative care across ICU settings improves symptom management, supports families, reduces non-beneficial interventions, and aligns care with patient values, without hastening death.
The model for how this integration is delivered will vary by setting, resources, and culture. In high-resource academic centers, embedded multidisciplinary palliative care teams and trigger-based consultation protocols represent the standard of care. In settings with limited specialist workforce, the primary palliative care model, in which intensivists themselves deliver core palliative competencies, is both evidence-based and achievable. The goal is not to replicate any single system’s approach but to ensure that every critically ill patient, wherever they are cared for, receives attention to their suffering, their values, and their dignity alongside attention to their physiology.
As ICU populations continue to age, as life-sustaining technologies advance, and as the complexity of critical illness increases, the integration of palliative care will only become more essential. Compassionate, goal-concordant, ethically grounded critical care is not a departure from excellence in intensive care medicine, it is its highest expression.
Ethical approval
This manuscript is a narrative review of published literature and does not involve human subjects, animal experiments, patient data, or clinical trials. Accordingly, ethics committee approval and informed consent were not required. No patient identifying information is included in this manuscript. The procedures described are consistent with the Helsinki Declaration of 1964, revised 2013.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Curtis JR, Kross EK, Stapleton RD. The importance of addressing advance care planning and decisions about do-not-resuscitate orders during novel Coronavirus 2019 (COVID-19). JAMA. 2020;323:1771-2. https://doi.org/10.1001/jama.2020.4894
- Aslakson RA, Curtis JR, Nelson JE. The changing role of palliative care in the ICU. Crit Care Med. 2014;42:2418-28. https://doi.org/10.1097/CCM.0000000000000573
- Kelley AS, Morrison RS. Palliative care for the seriously ill. N Engl J Med. 2015;373:747-55. https://doi.org/10.1056/NEJMra1404684
- Radbruch L, De Lima L, Knaul F, et al. Redefining palliative care-a new consensus-based definition. J Pain Symptom Manage. 2020;60:754-64. https://doi.org/10.1016/j.jpainsymman.2020.04.027
- World Health Organization (WHO). Palliative care. Geneva: WHO; 2020. Available at: https://www.who.int/news-room/fact-sheets/detail/palliative-care
- Worldwide Palliative Care Alliance; World Health Organization. Global Atlas of Palliative Care at the End of Life. 2nd ed. London: WPCA; 2020.
- Nelson JE, Azoulay E, Curtis JR, et al. Palliative care in the ICU. J Palliat Med. 2012;15:168-74. https://doi.org/10.1089/jpm.2011.9599
- Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46:e825-73. https://doi.org/10.1097/CCM.0000000000003299
- Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291:1753-62. https://doi.org/10.1001/jama.291.14.1753
- Quill TE, Abernethy AP. Generalist plus specialist palliative care-creating a more sustainable model. N Engl J Med. 2013;368:1173-5. https://doi.org/10.1056/NEJMp1215620
- Carson SS, Cox CE, Wallenstein S, et al. Effect of palliative care-led meetings for families of patients with chronic critical illness: a randomized clinical trial. JAMA. 2016;316:51-62. https://doi.org/10.1001/jama.2016.8474
- Lilly CM, De Meo DL, Sonna LA, et al. An intensive communication intervention for the critically ill. Am J Med. 2000;109:469-75. https://doi.org/10.1016/s0002-9343(00)00524-6
- Khandelwal N, Kross EK, Engelberg RA, Coe NB, Long AC, Curtis JR. Estimating the effect of palliative care interventions and advance care planning on ICU utilization: a systematic review. Crit Care Med. 2015;43:1102-11. https://doi.org/10.1097/CCM.0000000000000852
- Varelas PN, Abdelhak T, Hacein-Bey L. Withdrawal of life-sustaining therapies and brain death in the intensive care unit. Semin Neurol. 2008;28:726-35. https://doi.org/10.1055/s-0028-1105969
- Creutzfeldt CJ, Engelberg RA, Healey L, et al. Palliative care needs in the neuro-ICU. Crit Care Med. 2015;43:1677-84. https://doi.org/10.1097/CCM.0000000000001018
- Frontera JA, Curtis JR, Nelson JE, et al. Integrating palliative care into the care of neurocritically ill patients: a report from the improving palliative care in the ICU project advisory board and the center to advance palliative care. Crit Care Med. 2015;43:1964-77. https://doi.org/10.1097/CCM.0000000000001131
- Swetz KM, Freeman MR, AbouEzzeddine OF, et al. Palliative medicine consultation for preparedness planning in patients receiving left ventricular assist devices as destination therapy. Mayo Clin Proc. 2011;86:493-500. https://doi.org/10.4065/mcp.2010.0747
- Kavalieratos D, Gelfman LP, Tycon LE, et al. Palliative care in heart failure: rationale, evidence, and future priorities. J Am Coll Cardiol. 2017;70:1919-30. https://doi.org/10.1016/j.jacc.2017.08.036
- Gélinas C, Fillion L, Puntillo KA, Viens C, Fortier M. Validation of the critical-care pain observation tool in adult patients. Am J Crit Care. 2006;15:420-7.
- Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166:1338-44. https://doi.org/10.1164/rccm.2107138
- Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286:2703-10. https://doi.org/10.1001/jama.286.21.2703
- Sykes N, Thorns A. The use of opioids and sedatives at the end of life. Lancet Oncol. 2003;4:312-8. https://doi.org/10.1016/s1470-2045(03)01079-9
- Hiser SL, Fatima A, Ali M, Needham DM. Post-intensive care syndrome (PICS): recent updates. J Intensive Care. 2023;11:23. https://doi.org/10.1186/s40560-023-00670-7
- Putowski Z, Rachfalska N, Majewska K, Megger K, Krzych Ł. Identification of risk factors for post-intensive care syndrome in family members (PICS-F) among adult patients: a systematic review. Anaesthesiol Intensive Ther. 2023;55:168-78. https://doi.org/10.5114/ait.2023.130831
- Ramnarain D, Aupers E, den Oudsten B, Oldenbeuving A, de Vries J, Pouwels S. Post Intensive Care Syndrome (PICS): an overview of the definition, etiology, risk factors, and possible counseling and treatment strategies. Expert Rev Neurother. 2021;21:1159-77. https://doi.org/10.1080/14737175.2021.1981289
- Davidson JE, Jones C, Bienvenu OJ. Family response to critical illness: postintensive care syndrome-family. Crit Care Med. 2012;40:618-24. https://doi.org/10.1097/CCM.0b013e318236ebf9
- Azoulay E, Pochard F, Kentish-Barnes N, et al. Risk of post-traumatic stress symptoms in family members of intensive care unit patients. Am J Respir Crit Care Med. 2005;171:987-94. https://doi.org/10.1164/rccm.200409-1295OC
- Lautrette A, Darmon M, Megarbane B, et al. A communication strategy and brochure for relatives of patients dying in the ICU. N Engl J Med. 2007;356:469-78. https://doi.org/10.1056/NEJMoa063446
- White DB, Angus DC, Shields AM, et al. A randomized trial of a family-support intervention in intensive care units. N Engl J Med. 2018;378:2365-75. https://doi.org/10.1056/NEJMoa1802637
- Curtis JR, Engelberg RA, Wenrich MD, Shannon SE, Treece PD, Rubenfeld GD. Missed opportunities during family conferences about end-of-life care in the intensive care unit. Am J Respir Crit Care Med. 2005;171:844-9. https://doi.org/10.1164/rccm.200409-1267OC
- Kon AA, Davidson JE, Morrison W, et al. Shared decision making in ICUs: an American College of Critical Care Medicine and American Thoracic Society policy statement. Crit Care Med. 2016;44:188-201. https://doi.org/10.1097/CCM.0000000000001396
- Bernacki RE, Block SD; American College of Physicians High Value Care Task Force. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med. 2014;174:1994-2003. https://doi.org/10.1001/jamainternmed.2014.5271
- Childers JW, Back AL, Tulsky JA, Arnold RM. REMAP: A framework for goals of care conversations. J Oncol Pract. 2017;13:e844-50. https://doi.org/10.1200/JOP.2016.018796
- Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363:733-42. https://doi.org/10.1056/NEJMoa1000678
- Truog RD, Campbell ML, Curtis JR, et al. Recommendations for end-of-life care in the intensive care unit: A consensus statement by the American College of Critical Care Medicine. Crit Care Med. 2008;36:953-63. https://doi.org/10.1097/CCM.0B013E3181659096
- Luce JM, White DB. A history of ethics and law in the intensive care unit. Crit Care Clin. 2009;25:221-37, x. https://doi.org/10.1016/j.ccc.2008.10.002
- Penrod JD, Deb P, Dellenbaugh C, et al. Hospital-based palliative care consultation: effects on hospital cost. J Palliat Med. 2010;13:973-9. https://doi.org/10.1089/jpm.2010.0038
- Nelson JE, Bassett R, Boss RD, et al. Models for structuring a clinical initiative to enhance palliative care in the intensive care unit: a report from the IPAL-ICU Project (Improving Palliative Care in the ICU). Crit Care Med. 2010;38:1765-72. https://doi.org/10.1097/CCM.0b013e3181e8ad23
- Calton B, Abedini N, Fratkin M. Telemedicine in the time of Coronavirus. J Pain Symptom Manage. 2020;60:e12-4. https://doi.org/10.1016/j.jpainsymman.2020.03.019
- Johnson KS. Racial and ethnic disparities in palliative care. J Palliat Med. 2013;16:1329-34. https://doi.org/10.1089/jpm.2013.9468
- Sharma RK, Cameron KA, Chmiel JS, et al. Racial/ethnic differences in inpatient palliative care consultation for patients with advanced cancer. J Clin Oncol. 2015;33:3802-8. https://doi.org/10.1200/JCO.2015.61.6458
- Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med. 2007;167:453-60. https://doi.org/10.1001/archinte.167.5.453
- Nelson JE, Curtis JR, Mulkerin C, et al. Choosing and using screening criteria for palliative care consultation in the ICU: a report from the Improving Palliative Care in the ICU (IPAL-ICU) Advisory Board. Crit Care Med. 2013;41:2318-27. https://doi.org/10.1097/CCM.0b013e31828cf12c
- Ferrell BR, Dahlin C, Campbell ML, Paice JA, Malloy P, Virani R. End-of-life Nursing Education Consortium (ELNEC) Training Program: improving palliative care in critical care. Crit Care Nurs Q. 2007;30:206-12. https://doi.org/10.1097/01.CNQ.0000278920.37068.e9
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.