Abstract
Objective: A rare case of coinfection of Plasmodium falciparum and Aspergillus Fumigatus from travel to Tanzania is presented in this report.
Methods: A-43-year-old, Turkish male patient who travelled to Tanzania for business without any malaria prophylaxis was admitted to hospital with high fever (39.5 degrees C), weakness, nausea and vomiting and dyspnea when returned to Turkey. The patient had been treated in intensive care unite for sepsis and multi organ dysfunction as a result of the delayed malaria diagnosis. In addition to the presence of thrombocytopenia, anemia, metabolic acidosis, acute respiratory distress syndrome, hepatosplenomegaly and acute renal failure, aspergillus fumigatus emerged as a secondary opportunistic infection. Consent was obtained from the patient’s family to publish and all patient specific information has been identified, as a case report and negligible risk to the patient; formal ethics approval was not required because it posed negligible risk to the patient.
Results: He was treated with therapeutic plasma exchange seven times, prone position for 36 hours, continued renal replacement therapy for 72 hours, three cycles of artesunate, artemether lumefantrine for three days, with clindamycin and doxycycline. Additionally, meropenem for empirical antibiotherapy, and voriconazole and amphotericin b for Aspergillus were used.
Conclusion: This case report showed that malaria should be suspected in patients with febrile illness and that travel history to a malaria-endemic region and when fever recurs during the treatment process, secondary opportunistic infections should be considered in addition to malaria. Pulmonary aspergillosis can be seen in people with supressed immune systems and should also be considered in patients with plasmodium falciparum. Since it has been shown that complications may continue even after the parasite load is eliminated, the addition of extracorporeal treatments to antimalarial therapy may be effective in reducing mortality.
Keywords: invasive aspergillus, malaria, plasmodium falciparum, therapeutic plasma exchange
Introduction
Malaria is an important health problem that threatens public health and is endemic in tropical regions around the world. Early diagnosis and treatment of malaria reduces disease and prevents deaths. WHO recommends that all suspected cases of malaria be confirmed using parasite based diagnostic testing. Multiple medicines are used to treat malaria when a malaria parasite is resistant to a medicine (1). Invasive aspergillosis is usually detected in severely immunocompromised patients, but it has also been reported in patients with severe malaria due to transient immunosuppression by plasmodium falciparum (2,3). It has been reported that cases of association of Aspergillus and Plasmodium falciparum generally result in death (4,5).
Since Plasmodium falciparum affects erythrocytes of all ages, its parasitemia is high and typical fever attacks occur every 24-48 hours. Anemia secondary to the destruction of erythrocytes, jaundice and hepatosplenomegaly are observed during the seizure. It is possible to make a diagnosis with thin and thick blood films. In the treatment combination treatments of chloroquine, artesunate, artemether 20 mg and lumefantrine 120 mg are available. Doxycycline is also used in cases of chloroquine resistance. In cases of severe malaria, adjunctive therapies are employed alongside antimalarial treatment to manage life-threatening complications such as severe anemia, metabolic acidosis, hypoglycemia, and organ dysfunction. These supportive interventions include blood transfusions, fluid and electrolyte management, anticonvulsants, renal replacement therapy, and mechanical ventilation, tailored to the patient’s clinical condition.
In this case, the diagnosis and treatment process of opportunistic invasive aspergillosis secondary to Plasmodium falciparum malaria which was transmitted as a result of a trip to Tanzania, and treatment process of ARDS and multiple organ failure during intensive care follow up explained. We aim to prevent mortality and morbidity through early diagnosis and treatment in cases of Plasmodium falciparum malaria, which is rare in our country with this case study presentation.
Case Study
The patient, who was admitted to different hospitals for a week with symptoms of nausea, vomiting, weakness and persistent fever after returning from a trip to Tanzania, was admitted to our hospital due to increased respiratory distress. At the time of admission, he had tachypnea, thrombocytopenia, anemia, acute renal failure, metabolic acidosis, hepatosplenomegaly, confusion, severe fever (39.5 degrees C) and his Acute Physiology and Chronic Health Evaluation Score (APACHEII) was 11, Sequential Organ Failure Assessment (SOFA) Score was 10. The results of laboratory tests at admission and in next days are presented Table 1.
| This table reviews clinical laboratory values fort he index patient; Abbreviation: Wbc: White blood cell, rbc: red blood cells, alt: alanine aminotransferase, ast: aspartate aminotransferase, ldh: lactate dehydrogenase. | ||||||
| Table 1. Laboratory parameters of patient. | ||||||
| Parameters |
|
|
|
|
|
|
| C-reactive protein (0-5 mg/L) |
|
|
|
|
|
|
| Procalcitonin (<0.5 ng/mL) |
|
|
|
|
|
|
| Wbc (3.7-10.1 10e3/uL) |
|
|
|
|
|
|
| Platelet (155-366 10e3/uL) |
|
|
|
|
|
|
| Hemoglobin (12.9-15.9 g/dl) |
|
|
|
|
|
|
| Rbc (4.06-5.58 10e6/uL) |
|
|
|
|
|
|
| Creatinine (0.7-1.2 mg/dl) |
|
|
|
|
|
|
| Total bilirubin (<1.2 mg/dl) |
|
|
|
|
|
|
| Direct bilirubin (0-0.3 mg/dl) |
|
|
|
|
|
|
| Urea (17-43 mg/dl) |
|
|
|
|
|
|
| ALT (0-41 IU/L) |
|
|
|
|
|
|
| AST ( 0-37 U/L) |
|
|
|
|
|
|
| LDH (135-225 U/L) |
|
|
|
|
|
|
| pH (7.35-7.45) |
|
|
|
|
|
|
| PaO2 (75-100) |
|
|
|
|
|
|
| PaCO2 (35-45) |
|
|
|
|
|
|
| Be mmol/L |
|
|
|
|
|
|
| Lactate mmol/L(0.5-2) |
|
|
|
|
|
|
Taking under consideration his history of mosquito bite during the trip to Tanzania suggested malaria, the thick and thin blood films were performed and Plasmodium falciparum infection detected at the emergency service. Since there was multiple organ failure, he was taken to the intensive care unit for the treatment process. On admission to the intensive care unit he was tachypneic, oliguric, he required continuous catecholamine infusion and his Glasgow Coma Scale was 12. CT scan of the abdomen showed enlarged spleen and liver. Serological test Plasmodium falciparum antigen was positive.
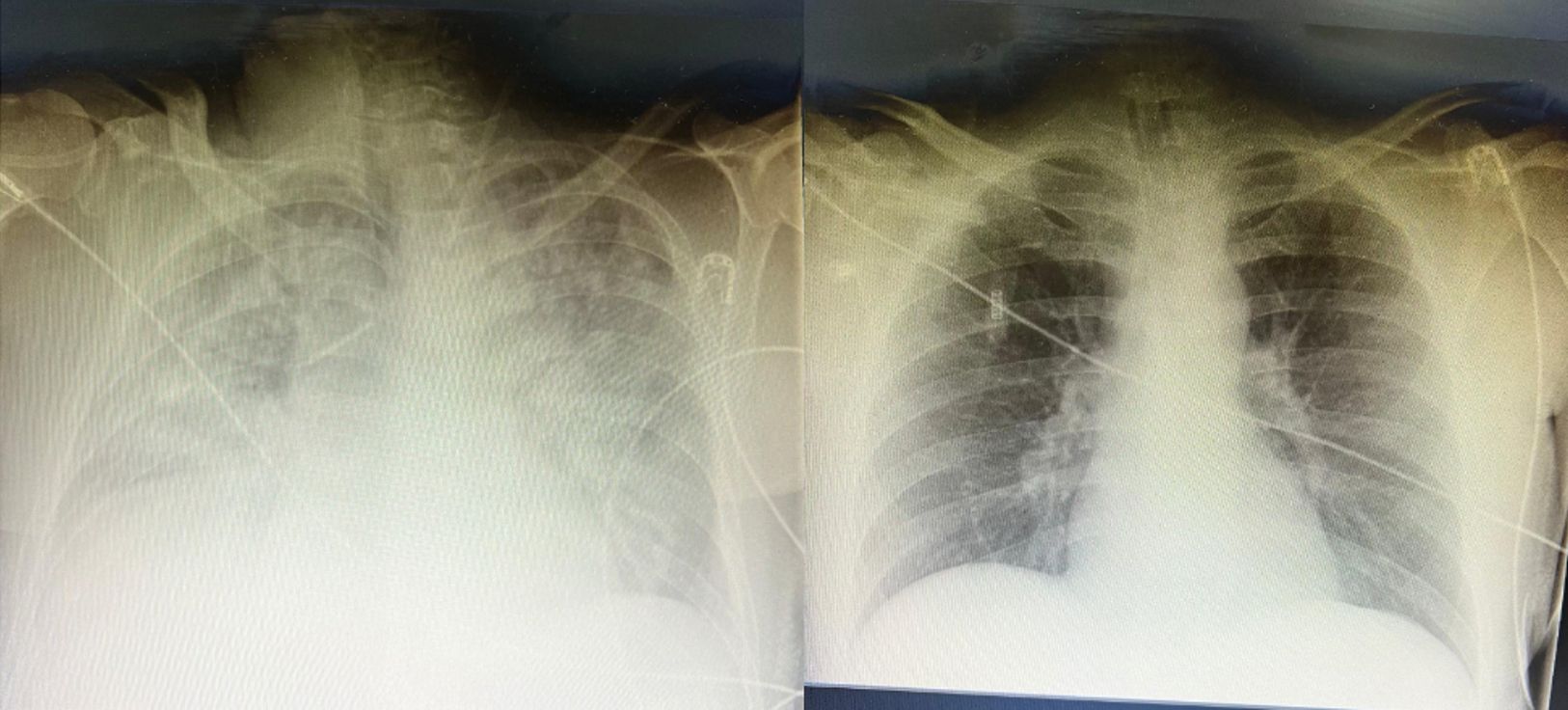
Treatment was initiated with 2.4 mg/kg artesunate and oxygen support, hydration for metabolic acidosis provided. On the second day he exhibited significant clinical deterioration, due to fever attacks, respiratory distress, increasing severity of renal failure and development septic shock (norepinephrine 1 mcg/kg/min and epinephrine 0.3 mcg/kg/min). He was intubated for severe acute respiratory distress syndrome (ARDS) Figure 1. Clindamycin 3x900 mg and meropenem 3x2gr were added as empirical antibiotics to his treatment. Continuous veno venous hemodiafiltration using an oxiris filter was applied in the treatment of septic shock-related acute kidney injury and external cooling therapy was applied for persistent fever. Since multi-organ failure developed with sepsis, therapeutic plasma exchange as immune adsorption treatment was started on the second day of intensive care admission (Table 2). Replaced plasma volume (1 plasma volume), fresh frozen plasma volume without anticoagulation was used for replacement fluid. As hemolysis continued and anemia developed, erythrocyte blood product transfusion was performed.
| Table 2. Therapeutic plasma exchange. | ||||||
| Device | Version | Manufacturer | Anticoagulant | Plasma volume treated | Replacement fluid | Number of frequency of procedures |
| Prismaflex TPE 2000 | 3.3 |
Baxter Healthcare/ Gambro Lundia AB, Swedish |
None | 1 | Fresh frozen plasma | 7 procedures, daily |
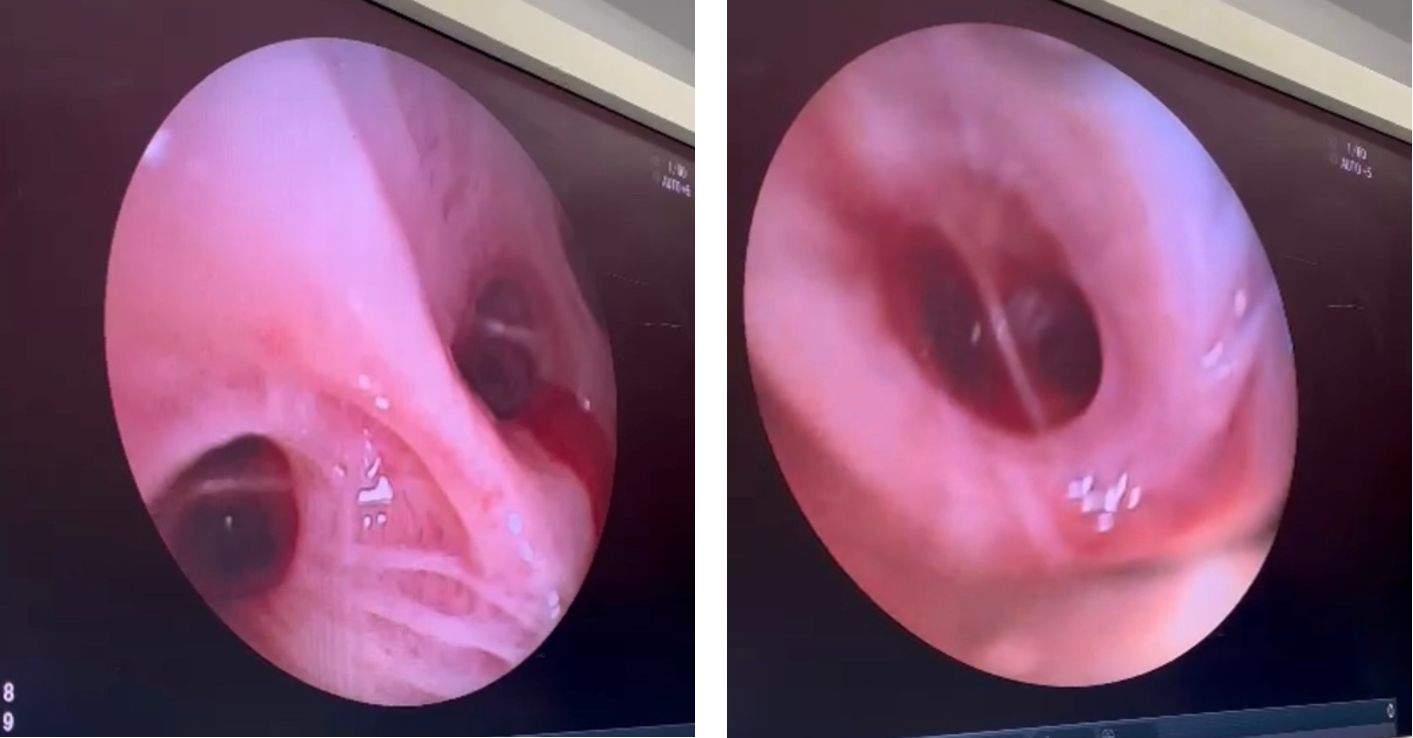
He was reentubated when Aspergillus- associated ARDS and then successfully extubated at the end of the 10th day after seven times therapeutic plasma exchange, 36 hours of prone position treatment for ARDS and 72 hours of CRRT. The renal function gradually improved. Clindamycin treatment (3x900 mg) was changed to doxycycline (200 mg /day) due to clinical worsening elevated LDH and an increase in febrile seizures under artesunate and chloroquine treatment. Artesunate treatment was extended to 9 days as 3 cures and at the end artemether 20 mg was combined with lumefantrine 120 mg treatment for 3 days in the form 2x4 tablets. After the treatment the control blood films were examined and the parasite load and antigen were studied and it was documented that the parasite load has ended. (Table 3). Upon the recurrence of fever after external cooling treatment, which was applied and terminated twice for 4 days, galactomannan was tested and resulted positive in the broncoalveolar lavage sampling performed considering the suspicion of secondary opportunistic infection to malaria aggravation and aspergillus fumigatus infection was detected in the tracheal aspirate that was taken. Flexible bronchoscopy was performed by thin mucus plugs with an intensively hemorrhagic appearance, bronchoalveolar lavage samples were obtained for microbiological and serological diagnosis (Figure 2). Treatment was continued with voriconazole 2x6 mg/kg loading dose followed by 2x4 mg/kg maintenance dose. On the fourth day of voriconazole treatment, voriconazole treatment was discontinued due to skin reaction and treatment with amphotericin b 3mg/kg was adjusted (Figure 3). As a result of the 18th day treatment, the patient was cured without secondary organ damage and transferred to the infection service and was later discharged home

Discussion
The rate of complicated malaria is high in P. Falciparum cases encountered in non endemic regions. Since the frequency of falciparum malaria resistance to antimalarial drugs is high, alternative extracorporeal treatments are used in intensive care units in complicated forms (6,7). Since it has been shown that complications may continue even after the parasite load is eliminated, the addition of extracorporeal treatments to antimalarial therapy may be effective in reducing mortality. In a review of 48 cases of complicated falciparum malaria, it was shown that mortality was reduced with the use of adjuvant plasmapheresis in addition to antimalarial treatment (8).
Aspergillosis is usually seen in immunocompromised patients, and it has a poor prognosis. Opportunistic fungal infections such as invasive aspergillosis, candidiasis and cryptococcal meningitis have been reported to be observed during falciparum malaria. Falciparum malaria can lead to suppression of both humoral and cellular immunity and also contributes to the deterioration of macrophage function. The reason for causing invasive fungal infections is due to the fact that macrophage monocytes and leukocytes are loaded with hemozoin and lose their phagocytosis ability (9). This macrophage suppression due to malaria occurs at the end of acute phase of the disease, and since it remains in the macrophages affected by hemozoin for several months, it can be observed in prolonged periods after recovery. This patient did not have a different comorbidity or neutropenia that supressed the immune system. The observation of aspergillosis at the stage when the parasite load decreases suggests that the supression of the immune system in the late phase secondary to malaria provides an environment for aspergillosis. Although the coexistence of malaria and aspergillus is rarely reported in the literature, malaria is more common in countries with limited resources, may be due to under reporting. Unlike the others, voriconazole and caspofungin were used together for aspergillosis in a case that did not result in death (3). In this case, voriconazole -related skin lesions were observed and amphotericin b was used instead.
Since this case was complicated and there was additional organ damage, both continuous veno venous hemodiafiltration therapy with oxiris filter and therapeutic plasma exchange were used, and mechanical ventilation support was used due to the due to the development of ARDS. Although the parasite load ended, the patient developed a secondary opportunistic infection, Aspergillus and its associated ARDS, as a result of the supression of the immune system. This mortal process was prevented with additional extracorporeal treatments.
Conclusion
We present a rare case of invasive Aspergillus in a patient with a previous Plasmodium Falciparum infection. In complicated Plasmodium Falciparum cases treated in intensive care units, the use of extracorporeal treatments should be considered in addition to antimalarial treatment to reduce parasite load and toxemia. Severe cases of P.falciparum malaria can be fatal even in individuals whose immune system is not supressed; in case of clinical worsening or recurrent fever, opportunistic fungal infections should be considered. Early diagnosis and rapid initiation of treatment are important for mortality and morbidity.
Ethical approval
Written informed consent was obtained from the patient legal represantatives.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- World Health Organization (WHO). Global malaria programme. WHO; 2024. Available at: https://www.who.int/teams/global-malaria-programme/guidelines-for-malaria (Accessed on Aug 21, 2024).
- Antonogiannaki EM, Proklou A, Tamiolakis D, Vassalou E, Kondili E. Invasive aspergillus tracheobronchitis in a patient with hairy cell leukemia and previous Plasmodium falciparum infection. Monaldi Arch Chest Dis. 2019;89:197-200. https://doi.org/10.4081/monaldi.2019.1055
- Eckerle I, Ebinger D, Gotthardt D, et al. Invasive aspergillus fumigatus infection after Plasmodium falciparum malaria in an immuno-competent host: case report and review of literature. Malar J. 2009;8:167. https://doi.org/10.1186/1475-2875-8-167
- Ruhnke M, Eichenauer E, Searle J, Lippek F. Fulminant tracheobronchial and pulmonary aspergillosis complicating imported Plasmodium falciparum malaria in an apparently immunocompetent woman. Clin Infect Dis. 2000;30:938-40. https://doi.org/10.1086/313819
- Hocqueloux L, Bruneel F, Pages CL, Vachon F. Fatal invasive aspergillosis complicating severe Plasmodium falciparum malaria. Clin Infect Dis. 2000;30:940-2. https://doi.org/10.1086/313814
- Hanif H, Shrestha B, Munankami S, et al. Severe malaria with a rare tetrad of blackwater fever, acute renal failure, disseminated intravascular coagulopathy, and acute acalculous cholecystitis. Case Rep Infect Dis. 2023;2023:5796881. https://doi.org/10.1155/2023/5796881
- Sithinamsuwan P, Sinsawaiwong S, Limapichart K. Guillain-Barre’s syndrome associated with Plasmodium falciparum malaria: role of plasma exchange. J Med Assoc Thai. 2001;84:1212-6.
- Chentsov VB, Tokmalaev AK, Kozhevnikova GM, Baranova AM, Vdovina ET, Emerole KC. Optimizing the intensive care treatment of severe and complicated Plasmodium falciparum malaria in nonimmune patients. J Trop Med. 2020;2020:1628270. https://doi.org/10.1155/2020/1628270
- Silveira EL, Dominguez MR, Soares IS. To B or not to B: understanding B cell responses in the development of malaria infection. Front Immunol. 2018;9:2961. https://doi.org/10.3389/fimmu.2018.02961
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.