Abstract
Objective: To evaluate the prognostic value of arterial pH at ICU admission for short-term survival after cardiac arrest.
Materials and Methods: This single-center observational study included 60 adults (≥18 years) admitted to the ICU between May 2024 and June 2025 after successful resuscitation with return of spontaneous circulation (ROSC). Clinical, demographic, and laboratory data were collected. Survivors and non-survivors at day 7 were compared using logistic regression and ROC analyses to determine independent predictors of mortality.
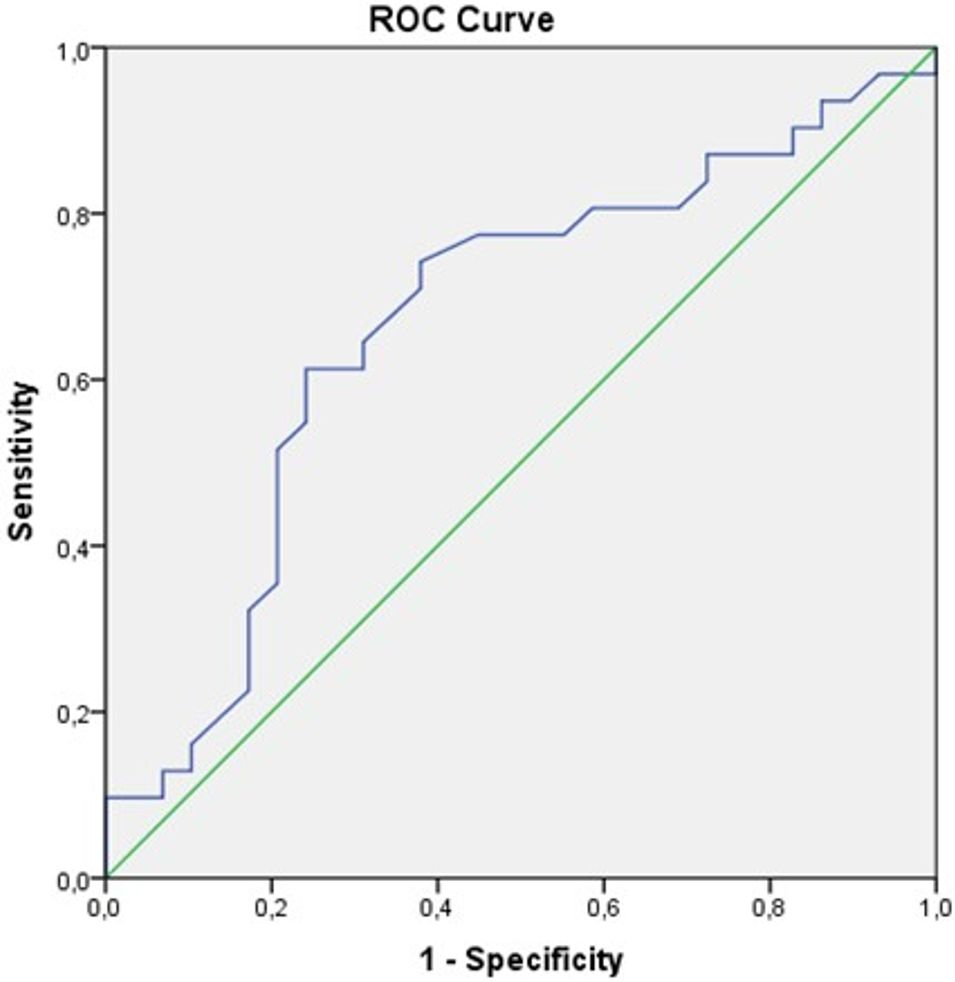
Results: The mean age was 61 ± 17 years, and 43% of patients were women. Seven-day mortality was 51.7%. Non-survivors were older and had higher APACHE II scores, lactate and procalcitonin levels, longer CPR-to-ROSC intervals, lower arterial pH values, and shorter ICU stays (all p < 0.05). In multivariable logistic regression analysis, age, higher APACHE II score, elevated procalcitonin levels, and lower arterial pH were independently associated with 7-day mortality. Lower arterial pH remained significantly associated with mortality (OR: 1.53; 95% CI: 0.93–2.86; p = 0.044). ROC analysis yielded an AUC of 0.668, with an optimal pH cut-off value of 7.13 (sensitivity 61.3%, specificity 75.9%).
Conclusion: Lower arterial pH at ICU admission independently predicts 7-day mortality after cardiac arrest, emphasizing the importance of early recognition and correction of acidosis in post-resuscitation care
Keywords: arterial blood gas, heart arrest, cardiopulmonary resuscitation, return of spontaneous circulation, critical care
Introduction
Despite substantial advancements in the management and care of cardiovascular conditions, sudden cardiac arrest (SCA) remains a formidable issue in both clinical cardiology and broader public health. Current estimates suggest that SCA contributes to approximately 15–20% of all deaths globally (1). Elevated mortality rates are noted not only in out-of-hospital cardiac arrest (OHCA) cases but also pose a significant challenge in in-hospital cardiac arrest (IHCA) scenarios. In the United States, the combined annual incidence of cardiac arrests including both OHCA and IHCA is estimated to range from 350,000 to 750,000 cases. Even with effective resuscitation and the restoration of spontaneous circulation (ROSC), the percentage of patients discharged alive from the hospital remains relatively low, estimated at approximately 18% (2). Although survival rates for in-hospital cardiac arrest in the United States demonstrated a marked improvement between 2000 and 2010, subsequent data indicate that these gains have plateaued, with current rates stabilizing around 25% in the years following 2010 (3). The fundamental goal of cardiopulmonary resuscitation (CPR) is to reestablish sufficient perfusion and oxygen delivery to vital organs—particularly the myocardium and brain—thereby sustaining cellular metabolism until spontaneous circulation is restored. Among the most critical factors influencing survival in these patients is the timely administration of high-quality, effective CPR (4). A range of clinical parameters has been recognized for their prognostic significance following cardiac arrest. These include the nature of the initial cardiac rhythm, patient age, existing comorbidities, both the duration and effectiveness of CPR efforts, the implementation of targeted temperature management when indicated, and various pre-arrest hematologic and biochemical indicators. Current investigations continue to examine brain biomarkers and other factors that may predict survival and favorable neurological outcomes in patients who achieve ROSC after resuscitation (5). This research examined the predictive significance of arterial pH levels—a biochemical marker of acid–base imbalance—on 7-day mortality in patients who underwent CPR and were thereafter admitted to the critical care unit (ICU).
Materials and Methods
This retrospective study was conducted in the intensive care unit of a tertiary medical center between May 2024 and June 2025. Adults (≥18 years) who experienced cardiac arrest, achieved return of ROSC, and remained in the ICU for at least 24 hours were included (n = 60). Data were extracted from electronic hospital records and medical charts, including age, sex, Glasgow Coma Scale after ROSC, APACHE II and SOFA scores, comorbidities, ICU stay length, mechanical ventilation duration, witnessed status, arrest location, collapse-to-ROSC interval, and need for sedation, renal replacement therapy, transfusion, or arrhythmia management. Laboratory parameters white blood cell count, hemoglobin, CRP, procalcitonin, arterial pH, lactate, bicarbonate, pCO2, albumin, creatinine, BUN, liver enzymes, and electrolytes were recorded. The primary endpoint was 7-day all-cause mortality. Ethical approval was obtained from the Institutional Review Board (Ref: 645; September 19, 2025), and informed consent was waived due to the study’s retrospective design.
Statistical analysis
Data were analyzed using SPSS version 22.0. Normality was assessed with the Shapiro–Wilk test. Continuous variables were expressed as mean ± standard deviation or median (interquartile range) as appropriate, and compared using the Student’s t-test or Mann–Whitney U test. Categorical variables were analyzed with the chi-square or Fisher’s exact test, depending on expected cell counts. Factors associated with 7-day mortality were evaluated by logistic regression, and the predictive value of arterial pH was examined using ROC analysis. The optimal cut-off value for arterial pH was determined using the Youden index. A two-tailed p value < 0.05 was considered statistically significant.
Results
Sixty patients met the inclusion criteria; 26 (43%) were female, and the mean age was 61 ± 17 years. The 7-day mortality rate was 51.7%. Median ICU stay was 5 days (IQR: 2–11). At admission, the mean APACHE II and median SOFA scores were 25 ± 6 and 10 (IQR: 8–12), respectively.
The underlying causes of cardiac arrest included acute coronary syndrome, malignant arrhythmias, pulmonary embolism, and respiratory arrest. Among these, acute coronary syndrome and arrhythmic causes constituted the most frequent etiologies, followed by pulmonary embolism and respiratory arrest. Patients with trauma-related cardiac arrest were not included in the study cohort.
Cardiac arrest occurred in-hospital in 17 patients (28%) and out-of-hospital in 43 (72%); 21 cases (35%) were witnessed. The median time from arrest to ROSC was 20 minutes (IQR: 15–40). Sedation was used in 46 patients (77%), blood product transfusion in 22 (37%), and arrhythmias occurred in 37 (62%).
Common comorbidities were hypertension (43%), diabetes mellitus (35%), coronary artery disease (32%), COPD (27%), chronic kidney disease (23%), and heart failure (22%). Cerebrovascular disease and atrial fibrillation were each observed in 3 patients (5%). Post-ROSC neurological assessment showed a median GCS of 3 (IQR: 3–4), and 16 patients (27%) required renal replacement therapy.
On admission, median lactate was 8 mmol/L (IQR: 5–12), arterial pH 7.16 (IQR: 6.9–7.26), pCO2 42 mmHg (IQR: 31–59), and HCO3 15 mmol/L (IQR: 6–15).
Non-survivors were older (67 ± 14 vs. 54 ± 17 years; p = 0.002) and had higher APACHE II scores (28 ± 5 vs. 22 ± 6; p = 0.001), lactate (10 [3–22] vs. 6 [1–18] mmol/L; p = 0.005), and procalcitonin levels (9 [0.04–25] vs. 1.9 [0.1–100] ng/mL; p = 0.001). CPR-to-ROSC time was longer in non-survivors (30 [10–60] vs. 15 [5–60] min; p = 0.003).
Arterial pH was lower in non-survivors (7.09 [6.5–7.35] vs. 7.22 [6.8–7.41]; p = 0.025), who also had shorter ICU stays (4 [2–7] vs. 11 [2–139] days; p = 0.001). No significant differences were observed in gender, SOFA score, renal replacement therapy, sedation use, GCS, transfusion, WBC, CRP, albumin, hemoglobin, electrolytes, or comorbidity profiles (all p > 0.05). Table 1 summarizes the main findings.
| AF: Atrial fibrillation, ALT: Alanine aminotransferase, APACHE II: Acute physiologic and chronic health evaluation, AST: Aspartate transaminase, CAD: Coronary artery disease, CHF: Congestive heart failure, COPD: Chronic obstructive pulmonary disease, CRF: Chronic renal failure, CRP: C-reactive protein, CVD: Cerebrovascular disease, DM: Diabetes mellitus, GCS: Glasgow coma scale, HTN: Hypertension, ICU: Intensive care unit, IHCA: In-hospital cardiac arrest, LOS: Length of stay, n: Number, p: Probability, PCT: Procalcitonin, ROSC: Return of spontaneous circulation, SOFA: Sequential organ failure assessment, WBC: White blood cell, y: Year. | ||||
| Table 1. Demographic and clinical characteristics of the patients | ||||
| Variables |
|
|
|
|
| Age, (y) |
|
|
|
|
| Male, n(%) |
|
|
|
|
| APACHE II score |
|
|
|
|
| SOFA score |
|
|
|
|
| IHCA, n(%) |
|
|
|
|
| WBC (103/µL) |
|
|
|
|
| Lactate (mmol/L) |
|
|
|
|
| CRP (mg/dL) |
|
|
|
|
| pH |
|
|
|
|
| HCO3 (mEq/L) |
|
|
|
|
| PCO2 (mmHg) |
|
|
|
|
| Hemoglobin (g/dL) |
|
|
|
|
| Sodium (mmol/L) |
|
|
|
|
| Potassium (mmol/L) |
|
|
|
|
| Chloride (mmol/L) |
|
|
|
|
| Urea (mg/dL) |
|
|
|
|
| Creatinine (mg/dL) |
|
|
|
|
| AST (U/L) |
|
|
|
|
| ALT (U/L) |
|
|
|
|
| Procalcitonin (ng/ml) |
|
|
|
|
| CPR-to-ROSC time (min) |
|
|
|
|
| LOS in ICU, days |
|
|
|
|
In multivariable logistic regression analysis, age, APACHE II score, procalcitonin levels, and arterial pH were independently associated with 7-day mortality. (Table 2). Among these variables, lower arterial pH remained significantly associated with mortality (OR 1.53; 95% CI 0.93–2.86; p = 0.044). ROC analysis demonstrated an AUC of 0.668 (95% CI 0.53–0.81; p = 0.026), with an optimal cut-off value of 7.13, yielding a sensitivity of 61.3% and a specificity of 75.9% (Figure 1).
| APACHE II: Acute physiologic and chronic health evaluation, CI: Confidence interval, OR: Odds ratio, p: Probability. | |||
| Table 2. Multivariable binary logistic regression modeling of parameters for 7 day mortality | |||
| Variables |
|
|
|
| Age |
|
|
|
| APACHE II score |
|
|
|
| Lactate |
|
|
|
| Procalcitonin |
|
|
|
| pH |
|
|
|
Discussion
Cardiac arrest remains a condition with high mortality, and effective cardiopulmonary resuscitation is essential to achieve return of spontaneous circulation (ROSC) as early as possible and to improve neurological outcomes. Following cardiac arrest, tissue hypoperfusion and hypoxia lead to increased anaerobic metabolism and lactate production, resulting in metabolic acidosis (4). In addition, impaired ventilation and gas exchange during and after resuscitation may contribute to concomitant respiratory acidosis.
This investigation focused on analyzing the association between arterial pH levels and 7-day mortality among patients receiving post-CPR care in a tertiary ICU, independent of underlying etiology. Despite intensive care efforts, pre-ICU cardiac arrest is associated with a markedly elevated mortality rate, often exceeding 90%. Analysis of these cases indicates that younger patients exhibit improved survival outcomes, particularly when timely and appropriate interventions are administered by trained medical personnel (6). Survival trends among patients who experienced non-cardiac arrest etiologies revealed that the majority of fatalities occurred within the first 48 hours following ICU admission. In this period, patient-based aggressive treatment that does not create a serious burden on the patient’s hemodynamic status is of great importance in terms of prognosis. Among the patients we included in the study, the deceased patient group had higher age, the median time from arrest to ROSC, lactate, procalcitonin and APACHE II score, while the LOS in ICU and pH value was lower. Although several clinical and biochemical variables were associated with early mortality, multivariable analysis demonstrated that arterial pH remained independently associated with 7-day mortality, alongside established predictors such as age, APACHE II score, and procalcitonin levels. In our cohort, patients who died had significantly higher age, lactate, APACHE II, and procalcitonin levels compared with survivors, findings that are in line with previously published studies (7-10). The prognosis of patients may be affected by the acidosis due to refractory shock that occurs in this post-CPR patient group whose management and treatment are already difficult (11). While acidosis is defined as a blood pH below 7.35, in cases of severe acidosis (pH < 7.2), different clinical outcomes such as vasodilation, decrease in myocardial contractile function and mean arterial pressure values, decreased response to vasopressor agents, microcirculatory deregulation, arrhythmia, potassium imbalance and mental instability can be observed (12). When the 30-day mortality rates of patients with severe acidosis were examined, values as high as 74.8%, 68% and 83% were observed in different studies (13,14). In our study, based on the ROC curve for pH value, a cut-off value of 7.13 was obtained. Although differences in HCO3 and pCO2 levels did not reach statistical significance, non-survivors exhibited higher pCO2 levels and markedly elevated lactate concentrations, supporting the presence of combined metabolic and respiratory acid–base disturbances in the early post-resuscitation period. Lactate concentrations were notably elevated in patients who did not survive, compared to those who were discharged alive. This finding further supports the contribution of metabolic acidosis due to tissue hypoperfusion in early post-resuscitation mortality. Accumulated anions due to acute renal failure, which is common in post-CPR patients may also cause significant changes in pH (15,16). Jamme et al. showed that pH and HCO3 had a significant effect on mortality, while pCO2 had no effect in their study on 826 patients diagnosed with IHCA (11). Shin et al. In their evaluation of OHCA cases, the authors reported that pH, pCO2, HCO3, and lactate levels exhibited statistically significant differences between non-survivors and survivors (17). Kim et al. showed that pH, PaCO2 and lactate levels differed significantly between a sustained ROSC and a non-ROSC group among patients with OHCA but did not show a significant association between pH and survival (18). Trepa et al. showed that among 60 patients with proven coronary artery disease who underwent OHCA, pH was significantly lower in those who died than in those who survived (19). In a systematic review and meta-analysis including 4077 OHCA patients, a pH value of 7.22 was associated with favorable survival outcomes (16). In our study, the median pH value in the survivors group was 7.22 (6.8-7.41). However, the threshold value for mortality in the ROC curve was 7.13 for pH, with a sensitivity of 61.3% and a specificity of 75.9%.
Limitations
This study was performed at a single medical center, potentially restricting the applicability of its results to broader populations. The study cohort included a heterogeneous patient population, comprising individuals with a range of underlying conditions such as cardiac, cardiothoracic, neurosurgical, trauma-related, pulmonary, and post-operative diagnoses.
Furthermore, the retrospective study design and relatively small sample size introduce inherent risks of selection and information bias that could not be entirely eliminated. As a result of the retrospective methodology, certain clinical variables potentially affecting both short- and long-term outcomes in post-cardiac arrest patients particularly those related to CPR quality, neurological status, and post-resuscitation interventions were not available for analysis and may have influenced the statistical interpretations.
Conclusions
The findings of this study reinforce the association between acid–base disturbances and increased short-term mortality in patients who undergo cardiopulmonary resuscitation. Lower arterial pH values observed among non-survivors likely reflect the combined impact of metabolic (predominantly lactic) and respiratory acidosis in the early post-resuscitation period. Rather than representing an isolated abnormality, arterial pH serves as an integrative marker of systemic hypoperfusion and impaired ventilation following cardiac arrest. These findings underscore the importance of comprehensive acid–base assessment and close monitoring during post-resuscitation care. Early recognition and management of acidosis may contribute to improved outcomes in this vulnerable patient population.
Ethical approval
This study has been approved by the Clinical Research Ethics Committee of Gazi Yaşargil Training and Research Hospital (approval date: 19.09.2025, number: 645). Written informed consent was waived due to the retrospective nature of the study.
Author contribution
Study conception and design: AD, SY; Data collection: AD, MC; Analysis and interpretation of results: AD, BSK; Draft manuscript preparation: AD; Critical revision of the manuscript: SY, MC, BSK. The authors reviewed the results and approved the final version of the article.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Marijon E, Narayanan K, Smith K, et al. The Lancet Commission to reduce the global burden of sudden cardiac death: a call for multidisciplinary action. Lancet. 2023;402:883-936. https://doi.org/10.1016/S0140-6736(23)00875-9
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation. 2022;145:e153-639. https://doi.org/10.1161/CIR.0000000000001052
- Okubo M, Komukai S, Andersen LW, et al. Duration of cardiopulmonary resuscitation and outcomes for adults with in-hospital cardiac arrest: retrospective cohort study. BMJ. 2024;384:e076019. https://doi.org/10.1136/bmj-2023-076019
- Olasveengen TM, Mancini ME, Perkins GD, et al. Adult Basic Life Support: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2020;142:S41-91. https://doi.org/10.1161/CIR.0000000000000892
- Hoiland RL, Rikhraj KJK, Thiara S, et al. Neurologic prognostication after cardiac arrest using brain biomarkers: a systematic review and meta-analysis. JAMA Neurol. 2022;79:390-8. https://doi.org/10.1001/jamaneurol.2021.5598
- Allyn J, Vandroux D, Jabot J, et al. Prognosis of patients presenting extreme acidosis (pH <7) on admission to intensive care unit. J Crit Care. 2016;31:243-8. https://doi.org/10.1016/j.jcrc.2015.09.025
- Pekkarinen PT, Ristagno G, Wilkman E, et al; FINNRESUSCI Study Group. Procalcitonin and presepsin as prognostic markers after out-of-hospital cardiac arrest. Shock. 2018;50:395-400. https://doi.org/10.1097/SHK.0000000000001087
- Issa MS, Grossestreuer AV, Patel H, et al. Lactate and hypotension as predictors of mortality after in-hospital cardiac arrest. Resuscitation. 2021;158:208-14. https://doi.org/10.1016/j.resuscitation.2020.10.018
- Kandilcik M, Arslan M, Öksüz H, et al. Evaluation of the factors affecting mortality after cardiac arrest - do lactate and procalcitonin concentrations have any implications? Eur Rev Med Pharmacol Sci. 2024;28:3430-8. https://doi.org/10.26355/eurrev_202405_36188
- Holmström E, Efendijev I, Raj R, Pekkarinen PT, Litonius E, Skrifvars MB. Intensive care-treated cardiac arrest: a retrospective study on the impact of extended age on mortality, neurological outcome, received treatments and healthcare-associated costs. Scand J Trauma Resusc Emerg Med. 2021;29:103. https://doi.org/10.1186/s13049-021-00923-0
- Jamme M, Ben Hadj Salem O, Guillemet L, et al. Severe metabolic acidosis after out-of-hospital cardiac arrest: risk factors and association with outcome. Ann Intensive Care. 2018;8:62. https://doi.org/10.1186/s13613-018-0409-3
- Greenberg KI, Lecker SH. Metabolic acidosis. Adv Kidney Dis Health. 2025;32:61-8. https://doi.org/10.1053/j.akdh.2025.01.012
- Gutgold A, Salameh S, Nashashibi J, Gershinsky Y. Prognosis of patients with extreme acidosis on admission to the emergency department: a retrospective cohort study. Am J Emerg Med. 2024;76:36-40. https://doi.org/10.1016/j.ajem.2023.10.054
- Saral Öztürk Z, Emektar E, Özen Olcay H, Akkan S, Çevik Y. Outcome of cardiac arrest and non-cardiac arrest patients with severe acidosis in the emergency department: a retrospective cohort study. Eurasian J Emerg Med. 2025;24:244-50. https://doi.org/10.4274/eajem.galenos.2025.78466
- Jeppesen KK, Rasmussen SB, Kjaergaard J, et al. Acute kidney injury after out-of-hospital cardiac arrest. Crit Care. 2024;28:169. https://doi.org/10.1186/s13054-024-04936-w
- Patel NT, Carr CT, Hopson CM, Hwang CW. Lactate and pH as independent biomarkers for prognosticating meaningful post-out-of-hospital cardiac arrest outcomes: a systematic review and meta-analysis. J Clin Med. 2025;14:2244. https://doi.org/10.3390/jcm14072244
- Shin J, Lim YS, Kim K, et al. Initial blood pH during cardiopulmonary resuscitation in out-of-hospital cardiac arrest patients: a multicenter observational registry-based study. Crit Care. 2017;21:322. https://doi.org/10.1186/s13054-017-1893-9
- Kim YJ, Lee YJ, Ryoo SM, et al. Role of blood gas analysis during cardiopulmonary resuscitation in out-of-hospital cardiac arrest patients. Medicine (Baltimore). 2016;95:e3960. https://doi.org/10.1097/MD.0000000000003960
- Trepa M, Bastos S, Fontes-Oliveira M, et al. Predictors of in-hospital mortality after recovered out-of-hospital cardiac arrest in patients with proven significant coronary artery disease: a retrospective study. J Crit Care Med (Targu Mures). 2020;6:41-51. https://doi.org/10.2478/jccm-2020-0006
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.