Abstract
Objective: Invasive pulmonary aspergillosis (IPA) is a life-threatening fungal infection that predominantly affects immunocompromised individuals. Environmental exposure to large amounts of construction dust following natural disasters may also increase the risk of invasive fungal infections. We aimed to present a fatal case of IPA that developed in an earthquake survivor rescued from prolonged entrapment under collapsed buildings.
Methods: A female earthquake victim with no known chronic disease or history of immunosuppressive therapy was admitted to the intensive care unit (ICU) after prolonged entrapment under rubble, cardiac arrest, and severe crush-related complications. Clinical findings, microbiological results, imaging studies, treatment course, and outcome were retrospectively reviewed.
Results: The patient developed septic shock, acute kidney injury requiring renal replacement therapy, and persistent respiratory failure. Despite broad-spectrum antimicrobial therapy, fever and hypoxemia persisted. Thoracic computed tomography revealed multiple pulmonary nodular lesions and consolidations suggestive of invasive fungal infection. Aspergillus fumigatus was isolated from endotracheal aspirate cultures on the 17th day of ICU admission. Voriconazole therapy was initiated; however, the patient died on the 35th day of ICU hospitalization.
Conclusion: IPA should be considered in critically ill survivors of natural disasters, even in the absence of classical host-related risk factors. Early recognition of invasive fungal infections in patients exposed to substantial environmental dust and debris may facilitate timely antifungal treatment and potentially improve outcomes.
Keywords: aspergillosis, earthquake, invasive fungal infection, mortality
Introduction
Invasive pulmonary aspergillosis (IPA) caused by a hyaline mold fungus Aspergillus is an important cause of mortality and morbidity in immunosuppressed patients. The prevalence of Aspergillus spp, is reported to be increasing in intensive care units (ICU) around the world (1). The incidence of IPA in ICU patients was determined to be 1-6.9%. IPA affects approximately 300,000 patients a year, and more than 30 million patients are thought to be at risk. The mortality rate of invasive aspergillosis can reach 80-90%, especially in immunocompromised patient groups. If diagnosis is delayed and severe neutropenia persists, death may occur in almost all cases. Aspergillus fumigatus and Aspergillus flavus are common agents in invasive infections, while Aspergillus niger is a rarely reported agent (2). Aspergillus species are common in nature and are found in soil, plants and flowers, household dust, building materials and on decomposing organic compounds. Its small spores can easily hang in the air and spread to the environment. Aspergillus infections are usually transmitted through the transmission of these spores into the respiratory tract. Spores grow in tissue and transform into hyphae, causing tissue invasion and widespread infection (3). The main clinical findings of IPA are dry cough, dyspnea, pleural chest pain, fever unresponsive to broad-spectrum antibiotic therapy, and pulmonary infiltrates. Less common clinical findings are hemoptysis, pleural effusion and pneumothorax (4). Invasive fungal infections have been increasingly detected as an infectious agent in ICU patients who are not immunosuppressed in recent years (5). Although Aspergillus species are rare, they are increasingly detected as an infectious agent. In this case, we aimed to discuss the presentation of a case of IPA who did not have a chronic disease and have been pulled alive from the rubble after the earthquake.
Case presentation
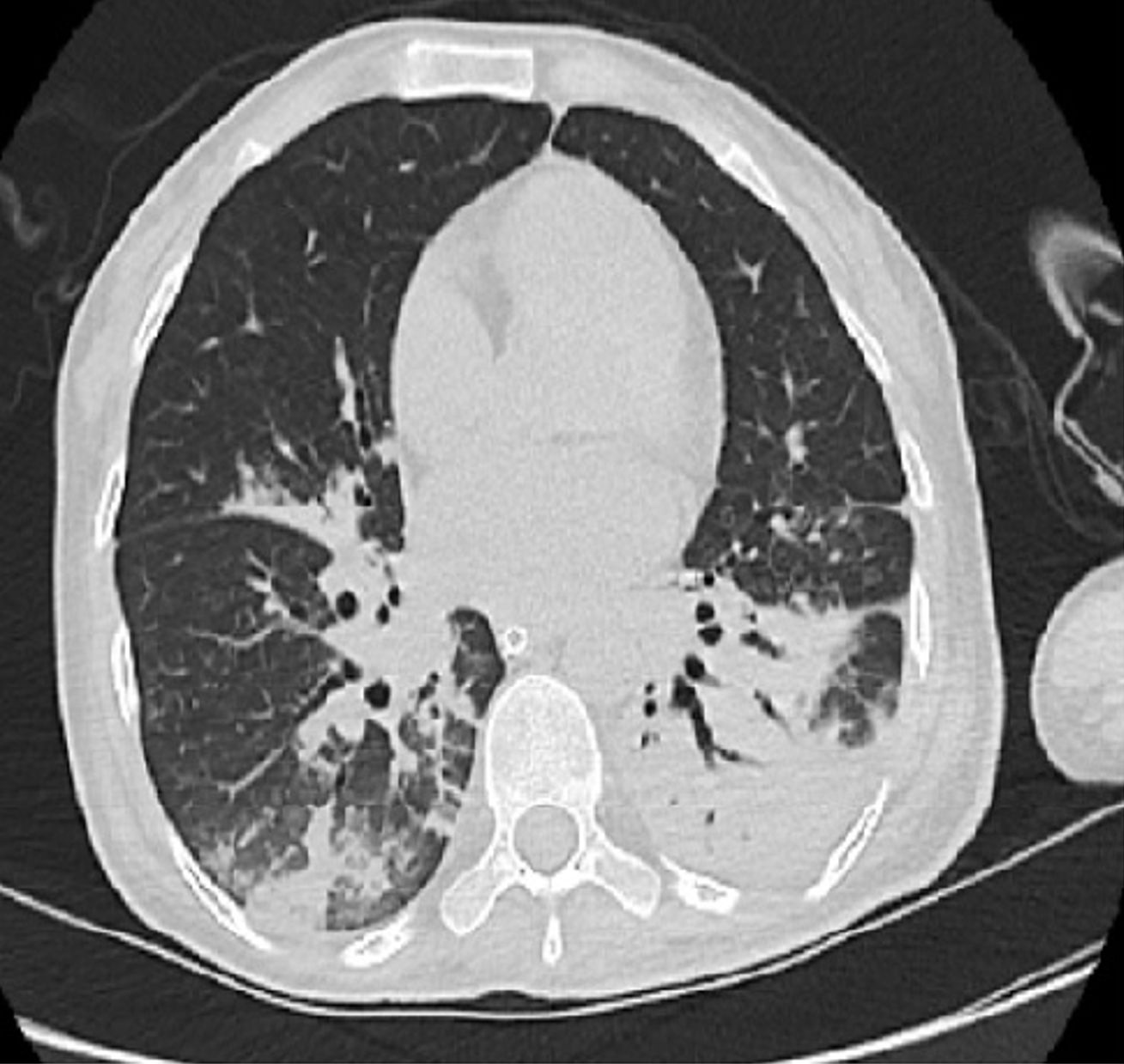
A female patient, who does not have any known chronic diseases and a history of drug use, was left under the rubble after the collapse of the building in which it is located during the earthquake on February 6, 2023. As a result of the search and rescue activities, the patient was pulled alive from the rubble (time to stay by collapsed building?) and was quickly transported to the nearest hospital by the 112 emergency service team. As a result of the development of cardiac arrest of unknown etiology in the hospital where she was taken, cardiopulmonary resuscitation was performed for 30 minutes. After the return of spontaneous circulation (ROSC) was obtained, invasive mechanical ventilator support was provided to the patient. Bilateral below-knee amputation was performed in the patient who developed necrosis due to compression of the lower extremities. Due to the patient’s need for advanced level ICU, she was transferred to the third level general ICU of our hospital. In the cranial, spinal, thoracic, abdominal and pelvic computed tomography (CT) scans of the patient done due to trauma, no fracture was observed in the bone structures. In the examination performed at the admission of the patient to the ICU, she was intubated and although she did not take sedative-hypnotic drug, she was unconscious and there was no cooperation and orientation. The pupil diameteres were normal size and bilateral pupils showed normal constriction when light was shown in the eyes. Bilateral lower extremities were amputated above the knee level and the wound site was clean, no purulent drainage and no necrotic tissue area. In other areas the skin integrity was intact, conjunctiva and oral mucosa were pallor, pulses were not felt sufficiently, heart sounds were normal, abdominal examination was normal and crepitan rales were heard in the lower zones of both lungs. Arterial blood pressure value 80/50 mmHg (under noradrenaline support at a dose of 0.5 mcg/kg/min), body temperature: 37.6 °C, breath: 20 times/min and heart rate: 110 beats / min and bedside ECG: sinus tachycardia. Laboratory values at first admission to the ICU: leukocytes: 10.200 /ul, hemoglobin: 7.5 mg/dl, neutrophils: 9170/ul, lymphocytes: 750/ul, platelets: 45.000/ul, CRP: 178 mg/dl, procalcitonin: 10 ng/ml, pH: 7.32, pCO2: 30 mmHg, HCO3: 15 mmol/L, pO2: 55 mmHg, sO2: 88%, urea: 95 mg/dL, creatinine: 3.4 mg/dL, sodium: 135 mEq/L, potassium: 5.27, phosphate: 5.2 mg/dL, mEq/L, AST: 602 U/L, ALT: 212 U/L, LDH: 1635 U/L, CK: 21267 U/L, and lactate: 1.39 mmol/L. The patient was anuric (24/h urine output was <100 ml). Due to increased renal function values, metabolic acidosis and hyperkalemia, the patient underwent intermittent hemodialysis and continuous veno-venous hemodialysis / hemodiafiltration as needed and according to her condition. In the diffusion-weighted MRI performed in the patient for hypoxic ischemic enfecephalopathy: At the centrum semiovale level, an appearance consistent with an acute infarct was observed which was hyperintense on diffusion-weighted imaging and hypointense on ADC maps. Follow-up, endotracheal aspirate, urine, central venous catheter and blood cultures were performed. Acinetobacter baumannii grew in endotracheal aspirate and methicillin-resistant Staphylococcus aureus was grown in the central venous catheter. Despite receiving broad-spectrum antibiotic treatment for gram-negative and gram-positive agents for a long time due to septic shock, a chest CT was performed due to persistent fever and low oxygen saturation values. In the CT report summary: patchy consolidation areas with air bronchogram and ground-glass opacity are observed in the right lung upper lobe posterior and middle lobe areas. In addition, there are widespread multiple nodular lesions, mostly in the right lung. When the findings were evaluated together, the CT result was interpreted in favor of pulmonary aspergillosis (Figure 1). On day 17 of ICU admission, endotracheal aspirate showed Aspergillus fumigatus. The patient received voriconazole treatment for 13 days due to IPA diagnosis, died on the 35th day of ICU while receiving voriconazole treatment.
Discussion
IPA is an opportunistic infection and occurs in some hosts where risk factors are present. In IPA cases, apart from malignant diseases and immunosuppressive cytostatic treatments, organ transplant recipients, underlying diseases such as diabetes, malnutrition, steroid use, uremia, haemodialysis patients, liver cirrhosis and chronic obstructive pulmonary disease have also been shown to pose a risk. Invasive aspergillosis is difficult to diagnose definitively (6). However, ICU patients who do not have known classical risk factors and for whom European Organisation for Research and Treatment of Cancer and the Mycosis Study Group Education and Research Consortium (EORTC/MSGERC) diagnostic criteria cannot be used are also at risk for IPA. In these patients, EORTC/MSGERC diagnostic criteria are not useful and in this study, AspICU criteria proposed by Blot et al were used in the diagnosis of IPA (7). According to AspICU criteria, growth of Aspergillus spp. in the lower respiratory tract sample is the entry criterion and patients with clinical and radiological findings worsening with classical host factors (neutropenia, hematological malignancy, bone marrow transplantation, corticosteroid use, etc.) are evaluated as having IPA (8). If the classical host factor is not present, pure Aspergillus spp. growth should be obtained from the bronchoalveolar lavage (BAL) sample (7). The importance of BAL sample is emphasized in many diagnostic algorithms or guidelines. This sample can be used not only for culture purposes but also for the detection of biomarkers such as galactomannan (GM), β-D-glucan and Aspergillus specific DNA (9-11). The sensitivity of these biomarkers in BAL sample is higher than in culture (12). Although valuable in diagnosis, BAL is not a frequently used sample. In serum/plasma samples, GM antigen test, Aspergillus PCR or β-D glucan test (BDG) tests can be performed. Positivities in these samples indicate invasive infection more strongly. Aspergillus PCR is not a test that can be performed in every center. Due to limited resources in our hospital, we diagnosed our patient with IPA based on aspergillus growth in endotracheal aspiration and suspicion of aspergillus pneumonia in thorax CT. Our patient had no history of any past medication use, including steroids, or chronic disease. There was no event or situation that would predispose the patient to the growth of aspergillus species, such as an aspergillosis outbreak in the hospital, a pandemic process, construction activities such as renovation, demolition, maintenance, excavation in and around the hospital, or fire. Cardiopulmonary arrest was observed in our patient. Pneumonia may occur in patients after cardiac arrest, but pneumonia due to aspergillosis has not yet been reported as a major complication (13). The first reported fungal outbreak associated with natural disasters began in 1985 with soft tissue infections caused by Rhizopus arrhizus in eight people following a volcanic eruption, and the frequency of these infections has increased steadily since then (14). A 68-year-old female patient who was followed up with the diagnosis of Tsunami Lung after the Great East Japan Earthquake in 2011, grew Aspergillus fumigatus on the 13th day of her stay in the ICU and the patient died on the 18th day (15). In 2005, aspergillus meningitis was observed in 5 pregnant women in Sri Lanka after cesarean section with spinal anesthesia due to the tsunami effect. The average incubation period was 11.2 days. Three patients died. Fungal cultures of four patients were positive for Aspergillus fumigatus.
In conclusion, after a chaotic environment such as an earthquake, where there may be many casualties and building demolitions, the prognosis for survivors in the hospital and intensive care unit may be poor due to the difficulty in obtaining appropriate diagnostic tools and the scarcity of trained professionals in mycology, little awareness, low research funding and lack of information. IPA is a disease with a high mortality rate in all conditions. Especially keeping in mind that fungal infections may also be a factor in pneumonia cases that may develop after natural disasters and studying appropriate methods to make the diagnosis within hospital possibilities can help increase the success of patient management and reduce mortality.
Ethical approval
Written consent could not be obtained because the patient’s relatives could not be reached by any via after she was hospitalized.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Spagnolo AM. Aspergillus contamination in healthcare facilities: an ever-present issue-prevention and control measures. Hygiene. 2025;5:1-13. https://doi.org/10.3390/hygiene5010003
- Chakrabarti A, Chatterjee SS, Das A, Shivaprakash MR. Invasive aspergillosis in developing countries. Med Mycol. 2011;49(Suppl 1):35-47. https://doi.org/10.3109/13693786.2010.505206
- Ledoux MP, Herbrecht R. Invasive pulmonary aspergillosis. J Fungi (Basel). 2023;9:131. https://doi.org/10.3390/jof9020131
- Patterson TF. Aspergillus species. In: Mandell GL, Bennett JE, Dolin R (eds). Mandell, Douglas and Bennett’s principles and practice of infectious diseases. 7th ed. Philadelphia: Churchill Livingstone; 2009:3241-55. https://doi.org/10.1016/B978-0-443-06839-3.00258-7
- De Pauw BE. Increasing fungal infections in the intensive care unit. Surg Infect (Larchmt). 2006;7(Suppl 2):93-6. https://doi.org/10.1089/sur.2006.7.s2-93
- Azim A, Ahmed A. Diagnosis and management of invasive fungal diseases in non-neutropenic ICU patients, with focus on candidiasis and aspergillosis: a comprehensive review. Front Cell Infect Microbiol. 2024;14:1256158. https://doi.org/10.3389/fcimb.2024.1256158
- Blot SI, Taccone FS, Van den Abeele AM, et al. A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am J Respir Crit Care Med. 2012;186:56-64. https://doi.org/10.1164/rccm.201111-1978OC
- Blot S, Rello J, Koulenti D. Diagnosing invasive pulmonary aspergillosis in ICU patients: putting the puzzle together. Curr Opin Crit Care. 2019;25:430-7. https://doi.org/10.1097/MCC.0000000000000637
- Verweij PE, Rijnders BJ, Brüggemann RJ, et al. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med. 2020;46:1524-35. https://doi.org/10.1007/s00134-020-06091-6
- White PL, Dhillon R, Cordey A, et al. A national strategy to diagnose coronavirus disease 2019-associated invasive fungal disease in the intensive care unit. Clin Infect Dis. 2021;73:e1634-44. https://doi.org/10.1093/cid/ciaa1298
- Koehler P, Bassetti M, Chakrabarti A, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021;21:e149-62. https://doi.org/10.1016/S1473-3099(20)30847-1
- Ullmann AJ, Aguado JM, Arikan-Akdagli S, et al. Diagnosis and management of aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin Microbiol Infect. 2018;24(Suppl 1):e1-e38. https://doi.org/10.1016/j.cmi.2018.01.002
- Perbet S, Mongardon N, Dumas F, et al. Early-onset pneumonia after cardiac arrest: characteristics, risk factors and influence on prognosis. Am J Respir Crit Care Med. 2011;184:1048-54. https://doi.org/10.1164/rccm.201102-0331OC
- Sipsas NV, Kontoyiannis DP. Occupation, lifestyle, diet, and invasive fungal infections. Infection. 2008;36:515-25. https://doi.org/10.1007/s15010-008-8129-5
- Kawakami Y, Tagami T, Kusakabe T, et al. Disseminated aspergillosis associated with tsunami lung. Respir Care. 2012;57:1674-8. https://doi.org/10.4187/respcare.01701
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.