Abstract
Objective: This case series aims to present the clinical characteristics, diagnostic processes, treatment strategies, and outcomes of patients with methanol intoxication treated in the intensive care unit (ICU).
Methods: Eight male patients, aged between 31 and 75 years, who were treated in the ICU for methanol intoxication within three weeks, were included. Their medical histories, clinical findings, laboratory results, treatments, and prognoses were described.
Results: The patients presented with a variety of symptoms such as visual loss, nausea, vomiting, abdominal pain, altered mental status, and respiratory distress. All patients had a history of consuming homemade alcohol, although in some cases the exact source and amount of alcohol were unknown. Arterial blood gas analyses revealed metabolic acidosis with elevated lactate levels. Negative blood ethanol levels, along with increased anion and osmolar gaps, supported the diagnosis of methanol intoxication. Patients received intravenous ethanol infusion, hemodialysis, and appropriate ICU supportive treatments. Three patients died (37.5%), while five survived.
Conclusion: This case series emphasizes the importance of prompt intervention in emergencies such as methanol intoxication. Early diagnosis and administering antidotes like ethanol and hemodialysis improve survival rates. Preventing the production of counterfeit alcohol and raising public awareness of its dangers should be key priorities.
Keywords: methanol intoxication, metabolic acidosis, anion gap
Introduction
Toxic alcohols are compounds that can induce severe systemic toxicity when ingested and are predominantly employed in industrial settings. Among them, methanol, isopropyl alcohol (isopropanol), and ethylene glycol represent the most frequent causes of poisoning. Methanol intoxication arises from the accidental or intentional ingestion of adulterated or illegally produced alcohol. Within the body, methanol is metabolized by alcohol dehydrogenase to formic acid (1). The formic acid concentration correlates directly with morbidity and mortality (2). Clinical manifestations of methanol poisoning may include nausea, vomiting, abdominal pain, confusion, visual impairment, acute renal failure, and coma (3,4). Diagnostic confirmation relies on a high index of suspicion in conjunction with laboratory and imaging findings, such as elevated osmolarity, severe high-anion gap metabolic acidosis, methanol levels, and cranial imaging (4,5). The therapeutic approach typically encompasses ethanol or fomepizole administration, hemodialysis, bicarbonate replacement, and folate supplementation (4-6). This case series aims to evaluate the clinical features, diagnostic modalities, therapeutic interventions, and outcomes of patients with methanol intoxication managed in our intensive care unit (ICU). The admission arterial blood gas parameters of all patients are summarized in Table 1.
| Table 1. Arterial blood gas analyses of the patients | ||||||||
| Parameters |
|
|
|
|
|
|
|
|
| pH |
|
|
|
|
|
|
|
|
| PaCO2 |
|
|
|
|
|
|
|
|
| PaO2 |
|
|
|
|
|
|
|
|
| HCO3 |
|
|
|
|
|
|
|
|
| BE |
|
|
|
|
|
|
|
|
| Lactate |
|
|
|
|
|
|
|
|
| Anion Gap |
|
|
|
|
|
|
|
|
Case 1
A 75-year-old male patient was admitted to the emergency department with confusion. His history indicated the ingestion of 200 ml of homemade alcohol. He had no notable past medical history. On examination, his overall condition was moderate, and he was conscious with a Glasgow Coma Scale (GCS) score of 14, although orientation and cooperation were impaired. Tachypnea and dyspnea were evident. Vital signs were as follows: heart rate 95 bpm, blood pressure (BP) 170/86 mmHg, SpO2 92% (room air). The initial arterial blood gas analysis demonstrated: pH 6.9, pCO2 25 mmHg, pO2 48 mmHg, base excess −24 mmol/L, lactate 12 mmol/L Anion gap was 24 mEq/L. The serum ethanol concentration was 18 mg/dl, and the urine ethyl glucuronide level exceeded 2000 ng/dl. Methanol intoxication was strongly suspected based on the increased anion and osmolar gaps, and intravenous ethanol therapy (10 cc/kg loading dose followed by 2 cc/kg/h maintenance infusion) was initiated. The patient was subsequently admitted to the ICU, where continuous venovenous hemodiafiltration (CVVHDF) was initiated. He was transferred to the internal medicine department on the third day of hospitalization.
Case 2
A 34-year-old male patient was admitted with an altered mental status. He had a history of alcohol consumption, although the source and quantity were unknown. His past medical history was unremarkable. On examination, his overall condition was poor, and he was unconscious, lacking orientation and cooperation. The pupils were mid-dilated. The GCS score was 3, and during cranial Computed Tomography (CT) imaging, cardiopulmonary resuscitation (CPR) was required for 5 minutes. The patient was subsequently transferred to the ICU. Initial arterial blood gas analysis demonstrated: pH 6.6, pCO2 35 mmHg, pO2 219 mmHg, base excess −28 mmol/L, lactate 9 mmol/L, with an anion gap of 26 mEq/L. Serum ethanol concentration was <10 mg/dl, and urine ethyl glucuronide exceeded 2000 ng/dl. Methanol intoxication was strongly suspected, and intravenous ethanol therapy (10 cc/kg loading dose, followed by 2 cc/kg/h maintenance infusion) was initiated. Due to hemodynamic instability requiring vasopressor support, CVVHDF was commenced. By the 7th hour of continuous renal replacement therapy (CRRT), the patient developed refractory metabolic acidosis, severe hyperlactatemia, and cardiac arrest. CPR was performed for 42 minutes. Following resuscitation, the patient was diagnosed with ischemic, hypoxic, and metabolic encephalopathy. Brain death was confirmed on the 7th day of hospitalization after a positive apnea test. The patient died on the 10th day of hospitalization.
Case 3
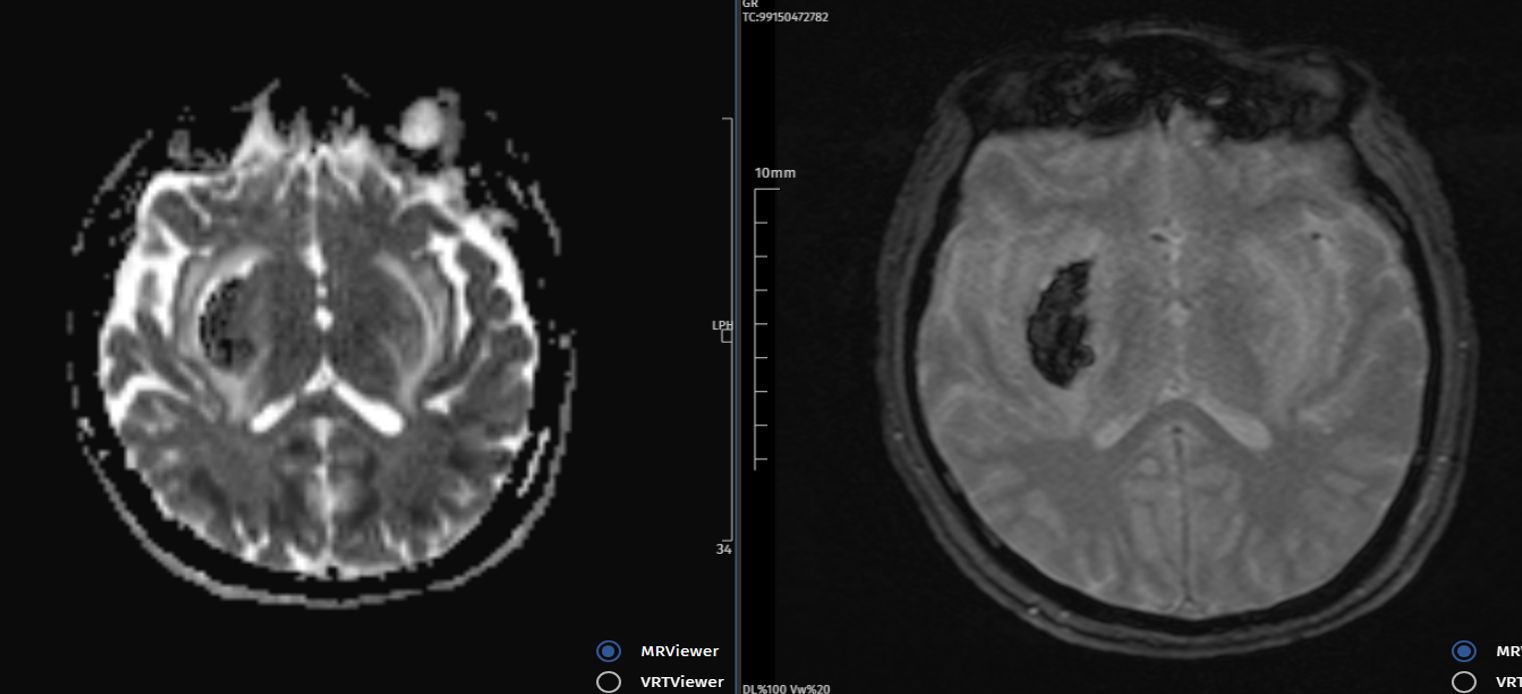
A 45-year-old male patient was admitted to the emergency department with acute vision loss, nausea, and respiratory distress. His history indicated alcohol ingestion from an unidentified source. He had no significant past medical history. On examination, his overall condition was poor, and he was unconscious, without orientation or cooperation. The pupils were isocoric. The GCS score was 8, and he subsequently developed worsening acidosis. The patient was intubated in the emergency department, and CPR was performed for 4 minutes. He was transferred to the ICU, where CVVHDF was initiated. Arterial blood gas analysis demonstrated: pH 6.85, pCO2 50 mmHg, pO2 115 mmHg, base excess −22 mmol/L, lactate 13 mmol/L. The anion gap was 31 mEq/L. Serum ethanol concentration was <10 mg/dl, and urine ethyl glucuronide exceeded 2000 ng/dl. Methanol intoxication was strongly suspected based on the elevated anion and osmolar gaps in conjunction with vision loss. Brain Magnetic Resonance Imaging (MRI) revealed hemorrhage in the right basal ganglion (Figure 1). On the 10th day of hospitalization, the patient underwent tracheostomy and was transferred to a secondary care ICU.
Case 4
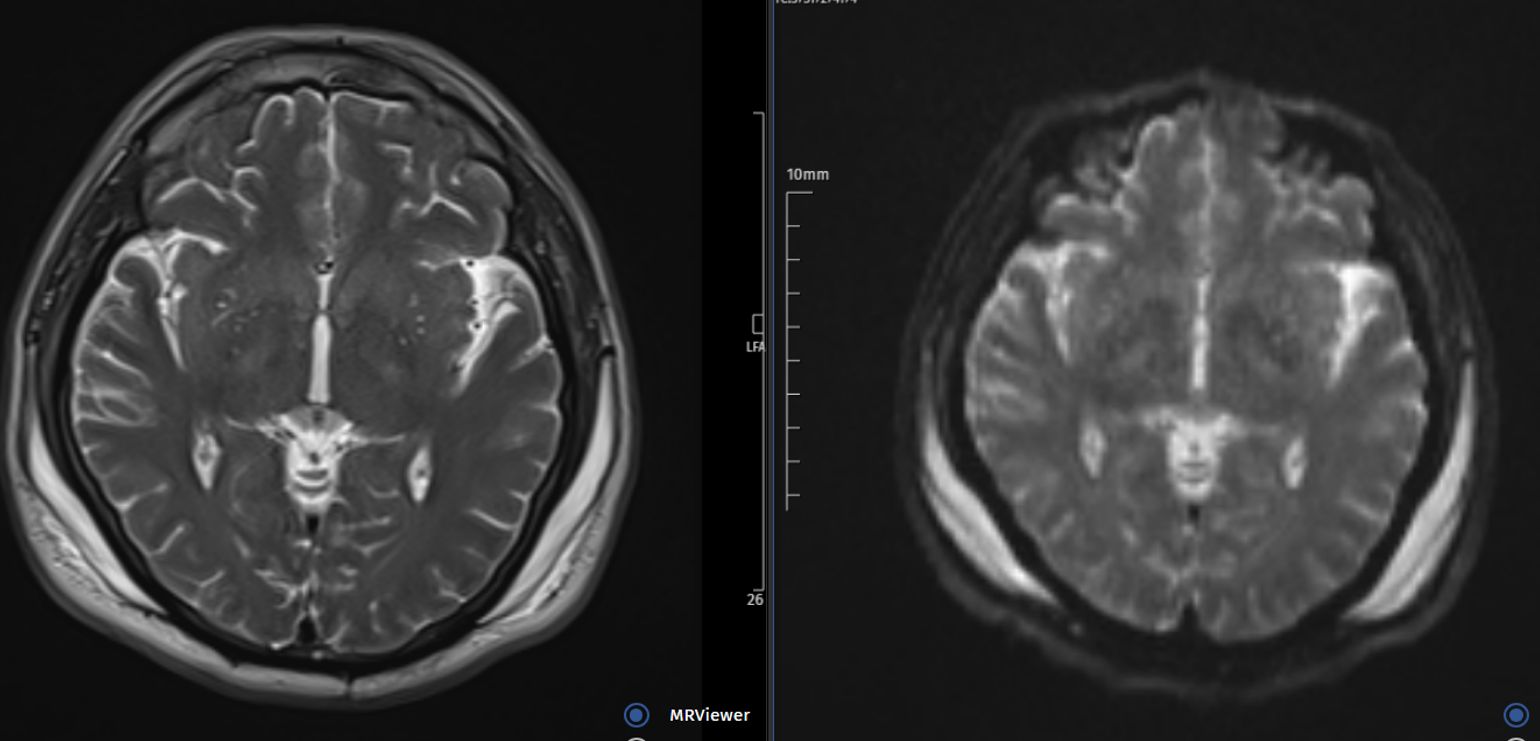
A 58-year-old male patient was admitted with head trauma and a history of alcohol consumption. According to his history, he had been assaulted after alcohol intake. He had no significant past medical history. On examination, his overall condition was poor, and he was confused, with impaired orientation and cooperation. The pupils were isocoric. The GCS score was 8. Following vomiting and aspiration, the patient was intubated in the emergency department. He was subsequently transferred to the ICU. Arterial blood gas analysis demonstrated: pH 7.31, pCO2 37 mmHg, pO2 58 mmHg, base excess −7 mmol/L, lactate 6.9 mmol/L. The anion gap was 28 mEq/L. Serum ethanol concentration was <10 mg/dl, and urine ethyl glucuronide exceeded 2000 ng/dl. Neurosurgical consultation was obtained, and acute neuropathology was not suspected on CT imaging. Methanol intoxication was considered based on the elevated anion and osmolar gaps together with altered mental status. CVVHDF was initiated in the ICU. Further imaging demonstrated diffusion restriction in the corpus callosum and bilateral basal ganglia (Figure 2). The patient subsequently underwent tracheostomy and was transferred to a secondary care ICU with a GCS score of 5.
Case 5
A 65-year-old male patient was admitted with vision loss. He reported ingestion of approximately 300 ml of alcohol from an unidentified source. He had no notable past medical history. On examination, his overall condition was moderate, and he was conscious, oriented, and cooperative. Vital signs were BP 170/110 mmHg, heart rate 85 bpm, SpO2 96%. Arterial blood gas analysis revealed: pH 7.14, pCO2 22 mmHg, pO2 48 mmHg, base excess −20 mmol/L, lactate 6.8 mmol/L. Following hemodialysis, the patient was transferred to the ICU. The anion gap was calculated as 25 mEq/L. Serum ethanol concentration was <10 mg/dl, while urine ethyl glucuronide exceeded 2000 ng/dl. Cranial imaging demonstrated no abnormalities. Based on the elevated anion and osmolar gaps together with vision loss, methanol intoxication was strongly suspected. The patient was observed in the ICU for 24 hours and subsequently discharged.
Case 6
A 64-year-old male patient was admitted with vision loss. His history revealed alcohol consumption from an unidentified source. He had a medical history of hypertension and coronary artery disease. During observation in the emergency department, he developed hypoventilation and required endotracheal intubation. On examination, his overall condition was poor, and his consciousness was sedated. Vital signs were as follows: blood pressure 135/52 mmHg (while receiving noradrenaline infusion at 1 mcg/kg/min), heart rate 79 bpm, SpO2 95%. Arterial blood gas analysis showed: pH 6.7, pCO2 62 mmHg, pO2 58 mmHg, base excess −24 mmol/L, lactate 6 mmol/L. He was transferred to the ICU, where CVVHDF was commenced. Despite ongoing vasopressor therapy, his blood pressure remained unstable, and he died following discontinuation of CVVHDF.
Case 7
A 47-year-old male patient was admitted to the emergency department with abdominal pain. His history indicated alcohol ingestion from an unidentified source. He had no notable past medical history. The patient was hemodynamically unstable and experienced a cardiac arrest following rapid deterioration. CPR was performed for 8 minutes, after which sinus rhythm was restored. He was subsequently transferred to the ICU. Arterial blood gas analysis demonstrated: pH 6.64, pCO2 36 mmHg, pO2 358 mmHg, base excess −28 mmol/L, lactate 13 mmol/L. Intravenous ethanol therapy was administered, and CVVHDF was initiated. Despite these interventions, the patient remained profoundly hypotensive and died 6 hours after ICU admission.
Case 8
A 31-year-old male patient was admitted to the emergency department with confusion. His history indicated consumption of homemade alcohol. He had no notable past medical history. On examination, his overall condition was moderate, and he was conscious, oriented, and cooperative. Vital signs were SpO2 92%, heart rate 92 bpm, and blood pressure 127/69 mmHg. The pupils were isocoric with a positive light reflex. Arterial blood gas analysis revealed: pH 7.0, pCO2 27 mmHg, pO2 55 mmHg, base excess −24 mmol/L, lactate 6.5 mmol/L. The anion gap was 14 mEq/L. Serum ethanol concentration was 18 mg/dl, and urine ethyl glucuronide exceeded 2000 ng/dl. Given the elevated anion and osmolar gap, methanol intoxication was strongly suspected, and the patient was admitted to the ICU. He received intravenous hydration and bicarbonate therapy. There was no indication for CVVHDF. He was transferred to the internal medicine department on the second day of hospitalization.
Discussion
This case series comprised eight patients who presented to the emergency department over 3 weeks with diverse clinical manifestations. The diagnoses were established based on strong clinical suspicion, elevated anion and osmolar gaps on arterial blood gas analysis, and negative serum ethanol concentrations. However, a definitive diagnosis of methanol poisoning necessitates advanced and costly techniques such as gas or liquid chromatography (7). Despite its diagnostic significance, methanol levels could not be measured in our hospital, and therefore, methanol toxicity could not be biochemically confirmed in blood samples.
All patients in our series were male, consistent with findings from previous studies (8). This phenomenon is considered to be attributable to the higher prevalence of illicit alcohol consumption among men in society. Rising alcohol prices and the increasing availability of illegally produced alcohol may have contributed to the consumption of counterfeit products.
In a retrospective study conducted in Turkey between 2002 and 2010, which included 383 fatalities due to methanol poisoning, it was reported that 64.7% (n=248) of the deaths occurred at home, 7.5% (n=29) in open areas, 9.9% (n=38) in other locations, and only 12.8% (n=49) in hospitals (9). In our case series, three of the eight patients died in the ICU, and two were palliative care patients with a diagnosis of metabolic encephalopathy. Our cohort’s observed mortality rate of 37% was comparable to the mortality rates reported in other outbreaks (28-48%) (10,11).
Ethanol was administered as an antidote in three of our patients. Owing to the high cost and limited availability of fomepizole, it was not utilized in the emergency department. Five of the eight patients underwent CVVHDF in the ICU, and one patient received hemodialysis in the emergency department. Considering the delay before ICU admission, early initiation of hemodialysis in the emergency department—without awaiting ICU transfer—may improve survival outcomes. A study conducted by Alhusain et al. reported a substantially lower mortality rate (17%), attributed to the initiation of fomepizole within the first 3 hours of hospital admission, followed by hemodialysis (12). In all cases, urine ethyl glucuronide levels exceeded 2000 ng/dl, whereas blood ethanol levels were negative. Only one patient demonstrated a serum ethanol concentration of 18 mg/dl. In this case, there was no indication of CVVHDF. Previous studies have shown that concurrent ingestion of ethanol and methanol attenuates clinical manifestations and prolongs the half-life of methanol (13,14).
In a retrospective cross-sectional study including 306 patients conducted in Iran during the COVID-19 pandemic, the most prominent neuroimaging findings associated with poor prognosis were hypodensity in the cerebellar nuclei, diffuse cerebral edema, and intracranial hemorrhage (15). In the neuroimaging of two patients diagnosed with metabolic encephalopathy and low GCS scores, intracranial hemorrhage and diffusion restriction in the basal ganglia were identified. However, basal ganglia lesions observed on imaging may not necessarily correlate with clinical outcomes, and putaminal lesions that resolve within one month following toxicity may not result in permanent functional impairment (16).
Based on this case series, we propose that a multidisciplinary approach to the diagnosis and management of methanol poisoning—emphasizing rapid identification and early initiation of hemodialysis—can substantially reduce morbidity and mortality. National diagnostic and therapeutic strategies warrant reevaluation, and new evidence-based guidelines should be developed. Furthermore, regulatory inspections must be strengthened, and public awareness regarding the dangers of counterfeit alcohol should be enhanced.
Ethical approval
Written informed consent was obtained from the patients’ legal representatives.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Jacobsen D, McMartin KE. Methanol and ethylene glycol poisonings. Mechanism of toxicity, clinical course, diagnosis and treatment. Med Toxicol. 1986;1:309-34. https://doi.org/10.1007/BF03259846
- Brent J, McMartin K, Phillips S, Aaron C, Kulig K, Methylpyrazole for Toxic Alcohols Study Group. Fomepizole for the treatment of methanol poisoning. N Engl J Med. 2001;344:424-9. https://doi.org/10.1056/NEJM200102083440605
- Kute VB, Godara SM, Shah PR, et al. Hemodialysis for methyl alcohol poisoning: a single-center experience. Saudi J Kidney Dis Transpl. 2012;23:37-43.
- Celik S, Karapirli M, Kandemir E, et al. Fatal ethyl and methyl alcohol-related poisoning in Ankara: A retrospective analysis of 10,720 cases between 2001 and 2011. J Forensic Leg Med. 2013;20:151-4. https://doi.org/10.1016/j.jflm.2012.05.009
- Jangjou A, Moqadas M, Mohsenian L, et al. Awareness raising and dealing with methanol poisoning based on effective strategies. Environ Res. 2023;228:115886. https://doi.org/10.1016/j.envres.2023.115886
- Roberts DM, Yates C, Megarbane B, et al. Recommendations for the role of extracorporeal treatments in the management of acute methanol poisoning: a systematic review and consensus statement. Crit Care Med. 2015;43:461-72. https://doi.org/10.1097/CCM.0000000000000708
- Ashurst JV, Nappe TM. Methanol toxicity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023. Available at: https://www.ncbi.nlm.nih.gov/books/NBK482121
- Aslan M, Özer D. Factors predicting mortality in methyl alcohol intoxication: A retrospective clinical trial. Med J Bakirkoy. 2024;20:48-54. https://doi.org/10.4274/BMJ.galenos.2023.2023.1-8
- Kurtas O, Imre KY, Özer E, et al. The evaluation of deaths due to methyl alcohol intoxication. Biomedical Research. 2017;28:3680-7.
- Md Noor J, Hawari R, Mokhtar MF, et al. Methanol outbreak: a Malaysian tertiary hospital experience. Int J Emerg Med. 2020;13:6. https://doi.org/10.1186/s12245-020-0264-5
- Paasma R, Hovda KE, Tikkerberi A, Jacobsen D. Methanol mass poisoning in Estonia: outbreak in 154 patients. Clin Toxicol (Phila). 2007;45:152-7. https://doi.org/10.1080/15563650600956329
- Alhusain F, Alshalhoub M, Homaid MB, Esba LCA, Alghafees M, Al Deeb M. Clinical presentation and management of methanol poisoning outbreaks in Riyadh, Saudi Arabia: a retrospective analysis. BMC Emerg Med. 2024;24:64. https://doi.org/10.1186/s12873-024-00976-1
- Barceloux DG, Bond GR, Krenzelok EP, Cooper H, Vale JA, American Academy of Clinical Toxicology Ad Hoc Committee on the Treatment Guidelines for Methanol Poisoning. American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. J Toxicol Clin Toxicol. 2002;40:415-46. https://doi.org/10.1081/clt-120006745
- Nanji AA. Absence of symptoms and acidosis in potentially lethal methanol poisoning. Ann Emerg Med. 1984;13:487. https://doi.org/10.1016/s0196-0644(84)80040-2
- Esmaeilian S, Teimouri A, Hooshmandi S, et al. Methanol poisoning during the COVID-19 pandemic in Iran: A retrospective cross-sectional study of clinical, laboratory, and brain imaging characteristics and outcomes. Health Sci Rep. 2023;6:e1752. https://doi.org/10.1002/hsr2.1752
- Hantson P, Duprez T, Mahieu P. Neurotoxicity to the basal ganglia shown by magnetic resonance imaging (MRI) following poisoning by methanol and other substances. J Toxicol Clin Toxicol. 1997;35:151-61. https://doi.org/10.3109/15563659709001186
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.