Abstract
Aims: Intentional drug overdose is a leading cause of poisoning-related intensive care admissions and a major concern in clinical toxicology and public health. Identifying toxicological patterns, demographic features, and associated outcomes is essential to guide prevention and optimize early management.
Methods: We conducted a retrospective analysis of toxicological profiles, psychiatric history, and clinical outcomes among patients admitted to the intensive care unit after intentional drug overdose. Data collected included demographics, psychiatric comorbidities, ingested drug classes, length of stay in the intensive care unit, need for mechanical ventilation, and mortality. Patients were categorized as single- or multiple-drug ingestion, and groups were compared using appropriate statistical tests.
Results: Among 229 patients (57.2% female; 59.1% aged 18–33 years), antidepressants (20.9%) and analgesics (17.3%) were the most frequent agents. Multiple-drug ingestion occurred in 65.9% and was associated with a longer intensive care unit stay (2.31 ± 2.61 vs. 1.60 ± 0.83 days; P = 0.0088). Mechanical ventilation was required in 3.1%, and mortality was 0.3%.
Conclusion: Intentional overdose predominantly affects young adults and often involves multiple-drug ingestion (acute polypharmacy). Although critical outcomes were rare, polypharmacy correlated with prolonged intensive care unit stay, supporting prevention efforts and targeted psychiatric follow-up.
Keywords: drug overdose, poisoning, intensive care units, length of stay, respiration, artificial, suicide, attempted
Introduction
Poisoning is a potentially life-threatening condition resulting from intentional or unintentional exposure to toxic agents. Such exposure may occur through suicidal ingestion of drugs or chemicals, accidental overdose, or inadvertent contact with environmental toxins. Clinical severity—and the attendant risks of morbidity and mortality—varies with patient age, the type and amount of substance ingested, and the time to presentation for medical care (1).
Drug ingestion is the most common method in suicide attempts presenting to emergency departments, with several reports noting rates exceeding 50% (2). Antidepressants and analgesics are among the pharmacologic agents most frequently implicated in these attempts (3).
Reported ICU admission rates for patients presenting with acute drug poisoning range from 3% to 40% (4).
Depending on the pharmacologic properties and dose of the ingested agent, respiratory failure may ensue, necessitating mechanical ventilation; prolonged ventilatory support can, in turn, increase ICU length of stay and mortality risk (5).
In this study, we retrospectively analyzed the demographics, ingestion patterns, need for mechanical ventilation, and mortality among patients admitted to the ICU after intentional drug overdose. We hypothesized that multiple-drug ingestion would be associated with a longer ICU stay and a higher risk of complications compared with single-drug ingestion.
Methods
We performed a retrospective chart review of adults admitted to the ICU for intentional drug ingestion between January 1, 2022 and January 1, 2025 (n = 229). Intentional ingestion was defined as self-reported or clinically documented consumption for self-harm/suicide, classified on the basis of emergency department (ED) notes and/or psychiatric consultation. Exclusions were recreational use, accidental overdose/medication error, unclear intent, incomplete records, or an indeterminate etiology of intoxication.
Ethical approval
This retrospective study was approved by the institutional ethics committee (Approval No: 2024/2-06) and conducted in accordance with the principles of the Declaration of Helsinki. Because only de-identified patient data were used, the requirement for informed consent was waived.
Outcomes
In this study, we used the term “multiple-drug ingestion” to denote the intentional ingestion of two or more pharmacologically distinct agents during a single suicide attempt. Although the term “polypharmacy” is classically defined as the chronic use of five or more medications, we adopted this terminology in a broader, descriptive sense to reflect acute exposure to multiple substances, consistent with prior toxicology literature. For clarity, we primarily use the term ‘multiple-drug ingestion’ for acute co-ingestion; ‘polypharmacy’ is used in a descriptive sense to refer to the same acute exposure context.
The primary outcome was ICU length of stay (LOS). Secondary outcomes included the need for mechanical ventilation, in-hospital mortality, and complications (e.g., renal replacement therapy). Explanatory variables comprised age, sex, psychiatric history, and ingested drug classes. Because only seven patients required mechanical ventilation and one patient died, multivariable logistic regression was underpowered; therefore, we conducted descriptive comparisons (e.g., by psychiatric diagnosis, polypharmacy, and drug type) between ventilated and non-ventilated patients.
Data collection and quality control
Two physicians with ICU/toxicology experience independently abstracted data using predefined criteria after standardized training. Inter-rater reliability was assessed in a random 10% sample, and discrepancies were resolved by consensus. Records missing critical variables (drug type, ICU duration, or outcomes) were excluded. This methodological framework follows established recommendations for rigorous retrospective chart review and is intended to enhance reproducibility and internal validity (6).
Psychiatric consultation notes were available for all patients admitted to the ICU and were systematically reviewed to extract information on psychiatric diagnoses, prior suicide attempts, substance use disorders, and post-discharge follow-up recommendations.
Toxicology
Confirmation of intent and substances relied primarily on clinical documentation. Urine toxicology was available in 56 of 229 patients (24.45%); among these, 52 of 56 (92.86%) were concordant with the reported agents (e.g., benzodiazepines, opioids, antidepressants, amphetamines, barbiturates), supporting the overall reliability of the data.
Urine toxicology screening was performed using a qualitative immunoassay panel capable of detecting common drug classes, including benzodiazepines, opioids, amphetamines, barbiturates, cocaine metabolites, and tricyclic antidepressants. Confirmatory testing by gas chromatography–mass spectrometry was not routinely available. Toxicology testing was ordered at the discretion of the treating physician and was not systematically performed in all patients.
ICU admission and treatment
According to institutional guidelines, ICU admission was recommended for patients evaluated by the ED physician or intensivist who met any of the following criteria: Glasgow Coma Scale (GCS) ≤ 12, respiratory rate < 10/min or oxygen saturation < 90% on room air, systolic blood pressure < 90 mmHg, clinically significant arrhythmias, severe metabolic acidosis (pH < 7.25), seizures, need for airway protection, ingestion of known high-risk agents (e.g., tricyclic antidepressants, opioids, organophosphates), or high imminent suicide risk as determined by psychiatric evaluation. Management followed standardized practices: gastric lavage (≤1 hour with a protected airway), activated charcoal (within 1–2 hours when not contraindicated), dialysis/hemofiltration for severe or dialyzable intoxications, mechanical ventilation for GCS ≤ 8 or respiratory failure, and antidotal therapy (e.g., naloxone, flumazenil) when indicated.
Gastric lavage was considered only within the first hour after ingestion and exclusively in patients with a protected airway, and it was contraindicated in caustic or hydrocarbon ingestion. Activated charcoal was administered within 1–2 hours when patients were alert or intubated and when bowel obstruction, ileus, or high aspiration risk was absent. Renal replacement therapy was reserved for severe intoxications involving dialyzable substances (e.g., lithium, methanol, ethylene glycol) or refractory metabolic derangements. Mechanical ventilation was initiated for GCS ≤ 8, respiratory failure, or loss of airway reflexes. Antidotal therapy (e.g., naloxone for opioids, flumazenil for benzodiazepines) was used selectively, with flumazenil avoided in patients with chronic benzodiazepine use or suspected mixed overdoses.
Statistical analysis
Because this was a retrospective chart review, no formal sample size calculation was performed; all eligible patients admitted during the study period were included. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA). Categorical variables were summarized as counts and percentages; continuous variables (e.g., laboratory parameters, length of stay) as mean ± standard deviation (SD). Group comparisons for categorical variables used Fisher’s exact or X² tests, as appropriate. Owing to non-normal distributions, differences in continuous variables between groups were assessed with the Mann–Whitney U test. Given the low frequency of certain outcomes (e.g., mechanical ventilation, mortality), inferences for these endpoints were interpreted with caution and considered exploratory rather than confirmatory. Statistical significance was set at P < 0.05. For sparse endpoints (e.g., mechanical ventilation, hemofiltration, mortality), proportions and exact 95% confidence intervals were calculated using the Clopper–Pearson method, prioritizing precision over model-based inference.
Results
Of the 229 patients included in the study, 131 (57.20%) were female and 98 (42.80%) were male. All met the inclusion criteria for intentional ingestion as defined in the Methods. Among those with available toxicology screening (n = 56), 92.80% had results consistent with their reported ingestion.
The majority of patients were young adults, with 59.10% aged between 18 and 33 years. Regarding seasonal distribution, admissions were most frequent during the summer months (31.40%, n = 72), followed by spring (23.60%, n = 54), autumn (23.10%, n = 53), and winter (21.80%, n = 50).
When admission times were analyzed, the highest frequency occurred between 20:00 and 04:00 (n = 88, 38.40%), followed by 14:00–20:00 (24.50%), 04:00–08:00 (21.00%), and 08:00–14:00 (16.20%) (Table 1).
| Presented as frequency (n) and percentage (%). | ||
| Table 1. Descriptive characteristics of the patients (N = 229) | ||
|
|
||
| Gender | Female |
|
| Male |
|
|
| Age | 18-25 years |
|
| 26-33 years |
|
|
| 34-41 years |
|
|
| ≥42 years |
|
|
| Psychiatric diagnosis | Yes |
|
| Chronic disease | Yes |
|
| Season of attempt | Spring |
|
| Summer |
|
|
| Autumn |
|
|
| Winter |
|
|
| Time of attempt | 08:00–14:00 |
|
| 14:00–20:00 |
|
|
| 20:00–04:00 |
|
|
| 04:00–08:00 |
|
|
| Pregnancy | Yes |
|
| Multiple suicide attempts | Yes |
|
| Alcohol or substance abuse | Yes |
|
There were no statistically significant differences between sexes with respect to age, season, or time of admission. However, a documented psychiatric diagnosis was significantly more common in males (27.55%) than in females (9.16%) (P < 0.05) (Table 2).
| *Statistical analysis was performed using Fisher’s Exact Test. Values with P < 0.05 were considered statistically significant. | ||||
| Table 2. Comparison of clinical and demographic features by gender (N = 229) | ||||
|
n (%) |
n (%) |
|
||
| Psychiatric diagnosis | Yes |
|
|
|
| Chronic disease | Yes |
|
|
|
| Season of attempt | Spring |
|
|
|
| Summer |
|
|
||
| Autumn |
|
|
||
| Winter |
|
|
||
| Time of attempt | 08:00–14:00 |
|
|
|
| 14:00–20:00 |
|
|
||
| 20:00–04:00 |
|
|
||
| 04:00–08:00 |
|
|
||
| Age | 18–25 years |
|
|
|
| 26–33 years |
|
|
||
| 34–41 years |
|
|
||
| ≥42 years |
|
|
||
The most frequently implicated agents in suicide attempts were antidepressants (20.88%; n = 52), analgesics (17.27%; n = 43), and antipsychotics (11.24%; n = 28), followed by alcohol co-ingestion (13.65%; n = 34), which was recorded as a concomitant intoxicant rather than a medication, antibiotics (8.84%; n = 22), over-the-counter cold and flu preparations (multi-ingredient) (7.63%; n = 19), and illicit substances (4.82%; n = 12). Less commonly involved were pesticides (2.41%), antiepileptics (2.81%), and various other agents (Table 3).
|
Presented as frequency (n) and percentage (%). Alcohol was recorded as a concomitant intoxicant rather than a medication. |
|
| Table 3. Distribution of ingested drug groups and concomitant intoxicants (N = 229) | |
|
|
|
| Antidepressant |
|
| Analgesic |
|
| Alcohol |
|
| Antipsychotic |
|
| Antibiotic |
|
| Cold and flu preparations (multi-ingredient, OTC) |
|
| Illicit substances |
|
| Antiepileptic |
|
| Others (e.g., antihypertensives, antiarrhythmics) and pesticides |
|
Of the patients, 65.94% (n = 151) ingested multiple drugs, while 34.06% (n = 78) took a single medication (Table 4).
| Values are presented as frequency and percentage. | ||
| Table 4. Overall clinical outcomes of the patients (N = 229) | ||
|
|
||
| Drugs | Single |
|
| Multiple |
|
|
| Mechanical ventilation support | Yes |
|
| Hemofiltration support | Yes |
|
| Mortality | Yes |
|
Seven patients (3.1%, 95% CI: 1.3–6.2) required mechanical ventilation—four in the single-drug group and three in the multiple-drug group—with no statistically significant between-group difference (P = 0.233). Hemofiltration was administered to two patients in the multiple-drug group (1.30%, 95% CI: 0.2–4.7) and to none in the single-drug group (95% CI: 0.0–4.6) (Table 5).
| Note: Fisher’s Exact Test was used for comparisons (N=78/N=151). P < 0.05 was considered statistically significant. Percentages are presented with 95% confidence intervals (Clopper–Pearson method). | |||
| Table 5. Clinical outcomes by number of ingested drugs | |||
|
|
|
|
|
| Mechanical ventilation support |
|
|
|
| Hemofiltration support |
|
|
|
Only one patient (0.33%) died during the study period—a 33-year-old man who developed respiratory failure following benzodiazepine overdose and required intubation. Although no sex-based mortality comparisons can be inferred from a single event, this finding is directionally consistent with prior evidence that completed suicides are more common in men.
No statistically significant differences were observed between the single- and multiple-drug groups in AST (median: 21 vs. 22), ALT (16 vs. 20), urea (22 vs. 21), or creatinine (0.80 vs. 0.70) (P > 0.05). CK levels were likewise similar (median: 114.5 vs. 125), although the maximum CK reached 1023 mg/dL in the multiple-drug group. Arterial blood gas analysis showed pH values within normal ranges in both groups; however, marked metabolic acidosis was identified in three intubated patients, which is clinically noteworthy (Table 6). The distribution of patients according to the number of ingested drugs is summarized in Table 7.
| Mann–Whitney U test was used. P < 0.05 was considered statistically significant. | |||
| Table 6. Comparison of biochemical parameters by drug intake type | |||
| Biochemical parameter |
Mean ± SD; Median (range) |
Mean ± SD; Median (range) |
|
| AST (U/L) |
|
|
|
| ALT (U/L) |
|
|
|
| Urea (mg/dL) |
|
|
|
| Creatinine (mg/dL) |
|
|
|
| CK (U/L) |
|
|
|
| Prothrombin time (PT), (sec) |
|
|
|
| pH (Arterial blood gas) |
|
|
|
| Lactate (mmol/L) |
|
|
|
| Multiple-drug ingestion was defined as the intentional ingestion of two or more pharmacologically distinct agents during a single suicide attempt. | |
| Table 7. Number of ingested drugs per patient (N = 229) | |
| Number of drugs ingested |
|
| 1 drug |
|
| 2 drugs |
|
| 3 drugs |
|
| 4 drugs |
|
| ≥5 drugs |
|
| Total |
|
As shown in Figure 1, ICU length of stay was significantly longer in the multiple-drug group. The mean ICU stay was 1.60 ± 0.83 days (median, 1; range, 1–4) for single-drug ingestion and 2.31 ± 2.61 days (median, 2; range, 1–16) for multiple-drug ingestion, with the difference reaching statistical significance (P = 0.0088).
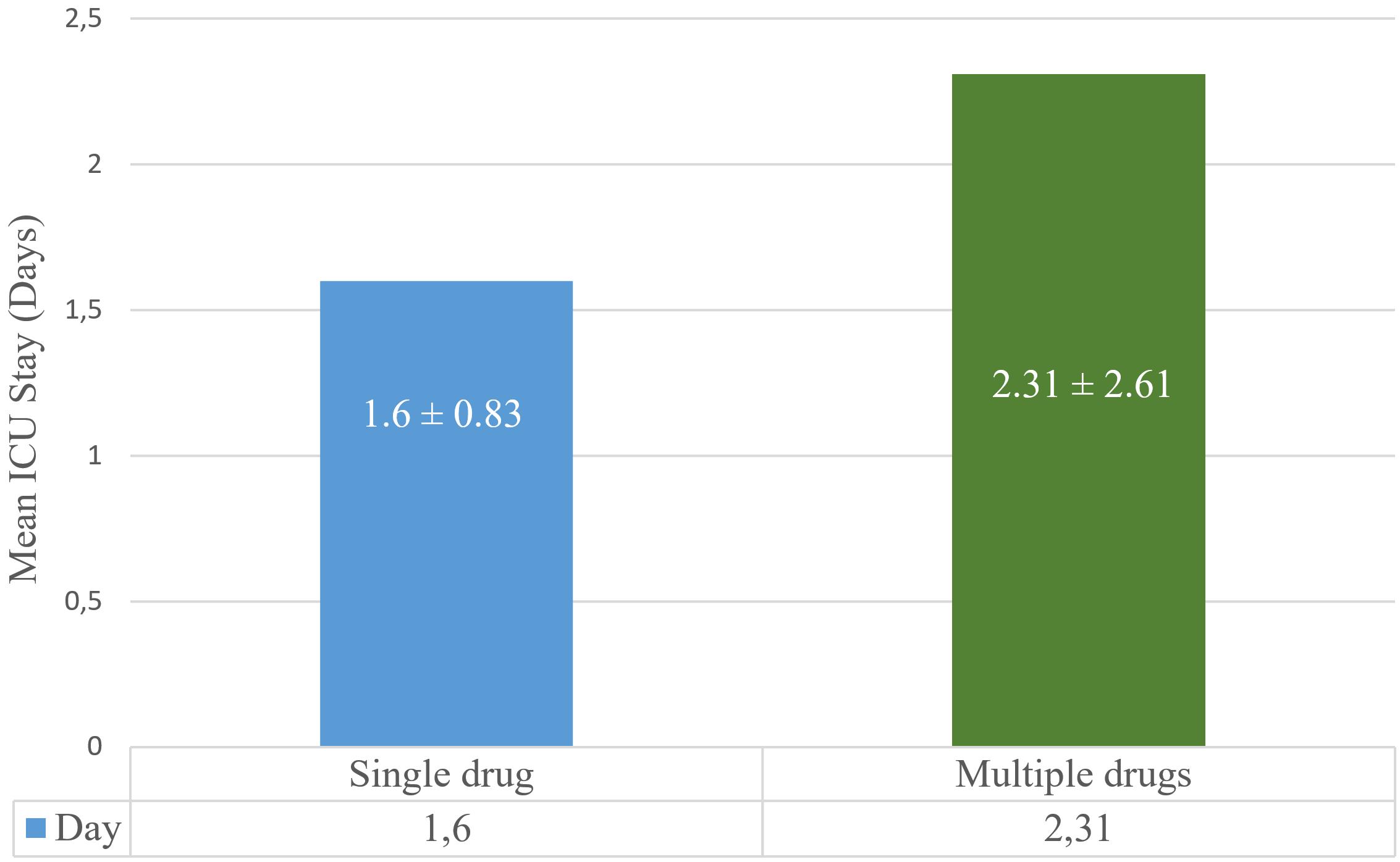
- Single drug: 1.6 ± 0.83; median (range): 1 (1–4)
- Multiple drugs: 2.31 ± 2.61; median (range): 2 (1–16)
- P = 0.0088*
- Mann–Whitney U Test. Values presented as mean ± standard deviation and median (min–max).
Discussion
The predominance of antidepressants and analgesics is consistent with pathophysiologic mechanisms that often necessitate ICU care: tricyclics can produce QRS widening and metabolic acidosis, whereas benzodiazepines depress respiratory drive—findings that align with our small but clinically relevant rate of mechanical ventilation. The limited acid–base disturbances observed likewise fit these expectations. Whether intentional or accidental, intoxication disrupts physiological homeostasis and is frequently managed in EDs and ICUs, imposing a substantial burden on healthcare systems and carrying a nontrivial risk of mortality (7).
Numerous studies have shown that the primary cause of intoxication is suicide attempts. Investigations by Tüfek et al. (8), Muhammedoğlu et al. (9), and Lee et al. (10) similarly demonstrated that drug-related poisonings most often result from suicidal intent.
Our findings are consistent with the literature regarding age and sex distribution. Multiple studies have reported that intoxication cases occur more frequently among young women (11,12) —a pattern also observed in our cohort. Notably, the only fatal case involved a male patient, aligning with prior evidence that completed suicides are more common in men (13).
A total of 26 patients had chronic illnesses. The reduced quality of life and increased psychological burden in such individuals may contribute to a higher risk of suicide. In line with prior ICU series, antidepressant-related intoxications were common in our cohort (14). In the study by Yeşiler et al. (15), more than one-third of cases carried a psychiatric diagnosis, and other reports similarly note high rates of depression and alcohol use disorder in comparable populations. Totoz et al. (16) and Wilcox et al. (17) likewise emphasized that most individuals who attempted suicide had a history of antidepressant use or a diagnosed psychiatric disorder. In our cohort, the overall prevalence of psychiatric disorders was 17.03%, increasing to 27.55% among male patients.
Suicide attempts during pregnancy and the postpartum period warrant particular attention. In our cohort, six patients were pregnant and twelve had a pregnancy within the preceding year, underscoring the psychological vulnerability of these stages. Enhanced psychosocial support during pregnancy and the postpartum period is therefore recommended.
A prior history of suicide attempts is a strong predictor of future self-harm (18). Structured interventions such as Safety Planning with follow-up can reduce subsequent suicidal behavior (19). In our study, 18 patients had a documented history of previous attempts, reinforcing the need for rigorous psychiatric follow-up after an initial event.
Although seasonal patterns vary across studies, our data showed a predominance in summer months, consistent with national statistics (20).
Approximately one-third of cases occurred during nighttime hours (20:00–04:00), when individuals are typically at home. This pattern suggests that attempts may not occur in isolation but rather in the presence of others.
Suicide attempts involving drug ingestion are well documented in the literature (2,3,9,15). The most frequently implicated classes are antidepressants and analgesics, likely reflecting their widespread use in the community and the ease of obtaining many such medications without a prescription. The ready availability of these agents in households may facilitate their use during psychological crises.
Although less commonly encountered, agents such as pesticides, antiepileptics, and over-the-counter multi-ingredient cold and flu preparations can also produce severe toxic effects. Clinicians should therefore remain vigilant not only for the most frequently used drugs but for all potentially harmful substances.
The reported rate of multiple-drug ingestion is high in the literature, and in our cohort it was 65.94% (21). This pattern may reflect both over-the-counter availability and the presence of multiple medications in households due to chronic disease. Restricting access to non-prescription drugs could help prevent such cases.
Reported ICU length of stay in the literature ranges from 1.7 to 2.5 days (18). In our study, LOS was 1.6 days in the single-drug group and 2.3 days in the multiple-drug group. This difference likely reflects the greater clinical complexity associated with polypharmacy.
Although the rate of mechanical ventilation was relatively low (3.06%), it falls within the range reported in prior studies (typically 3–20%). The lack of a statistically significant difference between groups likely reflects limited subgroup sample sizes. Larger studies are needed to more robustly evaluate these infrequent yet clinically critical outcomes.
Although the absolute numbers of mechanical ventilation and mortality were low, this pattern reflects the real-world epidemiology of drug intoxication in ICU settings. Reporting these outcomes—even in small numbers—adds to the cumulative evidence on patient profiles, risks, and clinical trajectories. Moreover, the concordance of our results with national registry data and prior literature supports their relevance despite limited statistical power.
Only two patients required hemofiltration, and there was a single fatality (0.33%). These findings support the notion that early admission and timely intervention can reduce mortality. Nevertheless, the multiorgan failure observed in the deceased patient underscores the potential severity of intoxication.
Reported mortality rates range from 0.92% to 4.20% (10). In our cohort, there was a single fatality—a male patient who developed multiorgan failure following benzodiazepine intoxication. All other intubated patients recovered and were discharged after treatment.
Morbidity and mortality in intoxication depend on multiple factors, including the type and dose of the toxic agent, pharmacokinetic properties, co-ingestion of other substances, baseline comorbid conditions, age, timeliness of medical intervention, adequacy of airway protection, and the development of complications such as metabolic acidosis, arrhythmias, or multiorgan failure (22). Accurate interpretation of biochemical and blood gas parameters is essential for the early detection of organ dysfunction. For example, tricyclic antidepressants can precipitate severe metabolic acidosis (23). Although our study did not identify significant between-group differences in routine biochemical measures, patients who required intubation exhibited notable laboratory derangements.
Most ICU admissions for intentional drug ingestion involved young women, with presentations clustering in the summer months and during nighttime hours. Antidepressants and analgesics were the most frequently implicated agents. Polypharmacy was associated with a longer ICU length of stay, whereas complication and mortality rates were low but not negligible. The predominance of these drug classes is consistent with established toxicodynamic risks—cardiotoxicity, metabolic acidosis, and central nervous system depression—which justify ICU-level monitoring in selected cases. These patterns should inform both clinical management and prevention. From a public health standpoint, safe prescribing, prudent regulation of over-the-counter access, secure home storage, pharmacy counseling for high-risk households, and early psychiatric follow-up may help reduce preventable overdose-related ICU admissions, particularly given the observed summer and nighttime clustering.
Limitations and future directions
This retrospective, single-center design relies on the accuracy of clinical documentation and limits generalizability. Although intent was classified using clinical records and psychiatric evaluation, misclassification is possible because toxicology screening was not universally available. Cases missing key variables (e.g., dose, duration of intoxication, comorbidities) were excluded, which may have introduced selection bias. The very low rates of critical outcomes (mechanical ventilation, 3.06%; mortality, 0.33%) constrained inferential analyses and rendered subgroup comparisons underpowered; consequently, multivariable adjustment for confounders was not feasible. Important determinants such as socioeconomic status, education, and prior psychiatric treatment were not captured. For rare outcomes, we report proportions with exact 95% confidence intervals to convey precision. Larger, multicenter prospective studies are needed to validate these findings and inform prevention strategies.
Conclusions
Intentional overdoses admitted to the ICU predominantly involved young adults and frequently featured polypharmacy. Although mortality and the need for mechanical ventilation were uncommon, polypharmacy was associated with a longer ICU stay, underscoring the need for targeted prevention and post-discharge psychiatric follow-up. Larger, multicenter prospective studies are warranted to confirm these observations.
From an intensive care perspective, our findings indicate that patients with multiple-drug ingestion constitute a higher-risk subgroup characterized by prolonged ICU length of stay and greater clinical complexity. Early identification of co-ingestion, structured toxicological screening, and anticipatory monitoring for respiratory and metabolic complications may facilitate more efficient resource utilization and earlier escalation of care when indicated. These results support the integration of standardized overdose pathways and mandatory psychiatric consultation into ICU protocols for intentional intoxication.
Ethical approval
This study has been approved by the Ethics Committee of Elazığ Fethi Sekin City Hospital (approval date: 24.10.2024, number: 2024/2-06). The requirement for informed consent was waived due to the retrospective design of the study.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Patel MM, Travers CD, Stockwell JA, Geller RJ, Kamat PP, Grunwell JR. Analysis of interventions required in 12,021 children with acute intoxications admitted to PICUs. Pediatr Crit Care Med. 2017;18:e281-9. https://doi.org/10.1097/PCC.0000000000001187
- Kawashima Y, Yonemoto N, Inagaki M, Yamada M. Prevalence of suicide attempters in emergency departments in Japan: a systematic review and meta-analysis. J Affect Disord. 2014;163:33-9. https://doi.org/10.1016/j.jad.2014.03.025
- Thanacoody R, Anderson M. Epidemiology of poisoning. Medicine (Baltimore). 2020;48:153-5. https://doi.org/10.1016/j.mpmed.2019.12.001
- Heyerdahl F, Bjornas MA, Hovda KE, et al. Acute poisonings treated in hospitals in Oslo: a one-year prospective study (II): clinical outcome. Clin Toxicol (Phila). 2008;46:42-9. https://doi.org/10.1080/15563650701210048
- Peñuelas O, Frutos-Vivar F, Fernández C, et al. Characteristics and outcomes of ventilated patients according to time to liberation from mechanical ventilation. Am J Respir Crit Care Med. 2011;184:430-7. https://doi.org/10.1164/rccm.201011-1887OC
- Gilbert EH, Lowenstein SR, Koziol-McLain J, Barta DC, Steiner J. Chart reviews in emergency medicine research: where are the methods? Ann Emerg Med. 1996;27:305-8. https://doi.org/10.1016/s0196-0644(96)70264-0
- Miniksar ÖH, Yıldız Miniksar D. Retrospective evaluation of adolescent drug intoxications followed in the intensive care unit. J Health Sci Med. 2020;3:203-8. [ https://doi.org/10.32322/jhsm.665105
- Tüfek D, Taşdemir BB, Sıvacı R. Retrospective investigation of intoxication cases followed up in intensive care unit. Turk J Intensive Care. 2017;15:67-71. https://doi.org/10.4274/tybdd.42243
- Muhammedoğlu N, Başaranoğlu G, Gül YG, Toptaş M, Baltalı S, Özütürk B. Evaluation of suicide and intoxication cases admitted to our newly opened intensive care unit. Medical Bulletin of Haseki. 2014;52:153-7. https://doi.org/10.4274/haseki.1766
- Lee HL, Lin HJ, Yeh STY, Chi CH, Guo HR. Presentations of patients of poisoning and predictors of poisoning-related fatality: findings from a hospital-based prospective study. BMC Public Health. 2008;8:7. https://doi.org/10.1186/1471-2458-8-7
- Sorge M, Weidhase L, Bernhard M, Gries A, Petros S. Self-poisoning in the acute care medicine 2005-2012. Anaesthesist. 2015;64:456-62. https://doi.org/10.1007/s00101-015-0030-x
- Dündar M, Mammadova N, Akyildiz BN. Demographic and clinical analysis of pediatric poisoning in intensive care. Annals of Medical Research. 2024;31:799-804. https://doi.org/10.5455/annalsmedres.2024.08.163
- Kim SH, Kim HJ, Oh SH, Cha K. Analysis of attempted suicide episodes presenting to the emergency department: comparison of young, middle aged and older people. Int J Ment Health Syst. 2020;14:46. https://doi.org/10.1186/s13033-020-00378-3
- Erol MK, Karahan MA, Altay N, Büyükfırat E. Retrospective analysis of cases diagnosed with acute poisoning due to antidepressant drug use in intensive care unit. Journal of Harran University Medical Faculty. 2018;15:226-9.
- Yeşiler Fİ, Şendur ÜG, İnan Demiroğlu G. Analysis of acute intoxication cases in intensive care unit. Aegean Journal of Medical Sciences. 2019;2:14-8. https://doi.org/10.33713/egetbd.472719
- Totoz T, Türk HŞ, Sayın P, Çınar S, Yıldırım Ç, Oba S. Retrospective analysis of intoxicated patients in our intensive care unit. Sisli Etfal Hastan Tip Bul. 2013;47:63-6. https://doi.org/10.5350/SEMB2013470204
- Wilcox HC, Conner KR, Caine ED. Association of alcohol and drug use disorders and completed suicide: an empirical review of cohort studies. Drug Alcohol Depend. 2004;76 Suppl:S11-9. https://doi.org/10.1016/j.drugalcdep.2004.08.003
- Ilgen MA, Harris AHS, Moos RH, Tiet QQ. Predictors of a suicide attempt one year after entry into substance use disorder treatment. Alcohol Clin Exp Res. 2007;31:635-42. https://doi.org/10.1111/j.1530-0277.2007.00348.x
- Stanley B, Brown GK, Brenner LA, et al. Comparison of the safety planning intervention with follow-up vs usual care of suicidal patients treated in the emergency department. JAMA Psychiatry. 2018;75:894-900. https://doi.org/10.1001/jamapsychiatry.2018.1776
- Turkish Statistical Institute. Ölüm ve ölüm nedeni istatistikleri, 2023. Available at: https://data.tuik.gov.tr/Bulten/Index?p=Olum-ve-Olum-Nedeni-Istatistikleri-2023-53709 (Accessed on Jun 4, 2025).
- Yılmaz Y, İnal FY, Toptaş M, Gürelik B, Erşan İ. Retrospective evaluation of intoxication cases presented to Sivas Numune Hospital. Medical Bulletin of Haseki. 2013;51(4):178-82. https://doi.org/10.4274/Haseki.1247
- Calcaterra SL, Severtson SG, Bau GE, et al. Trends in intentional abuse or misuse of benzodiazepines and opioid analgesics and the associated mortality reported to poison centers across the United States from 2000 to 2014. Clin Toxicol (Phila). 2018;56:1107-14. https://doi.org/10.1080/15563650.2018.1457792
- Khalid MM, Waseem M. Tricyclic antidepressant toxicity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. Available at: http://www.ncbi.nlm.nih.gov/books/NBK430931 (Accessed on Jun 4, 2025).
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.